
Translate this page into:
A Rare Potential Cause of Extraluminal Left Main Compression in ASD: An Echocardiographic Illustration
Ramesh Chand Kashav, MD Department of Cardiac Anaesthesia Atal Bihari Vajpayee Institute of Medical Sciences (ABVIMS) and Dr. Ram Manohar Lohia Hospital, Baba Kharak Singh Marg, New Delhi 110001 India drkashav@yahoo.co.in
This article was originally published by Thieme Medical and Scientific Publishers Pvt. Ltd. and was migrated to Scientific Scholar after the change of Publisher.
While atrial septal defect (ASD) classifies as the most common cause of grown-up congenital heart (GUCH) disease, it can present with unconventional symptoms, owing to the underlying pathophysiological alterations.1Atypical chest pain in ASD can be due to arrhythmias, right ventricular dysfunction, or ischemia. However, we describe an interesting echocardiographic finding, showcasing a rare potential cause of left main coronary artery (LMCA), resulting in chest pain in patients with ASD.
Although asymptomatic survival to adulthood is common, patients can present with pulmonary arterial enlargement, owing to varying degrees of pulmonary arterial hypertension. This can result in grossly distended pulmonary arteries. The left main coronary artery arises just above the left Sinus of Valsalva and courses behind the pulmonary trunk. It travels for a very short distance along the epicardium between the pulmonary trunk and aorta before dividing into anterior descending and circumflex arteries.2 The expansion of pulmonary artery can manifest as a cause of extraluminal/dynamic LMCA compression.3-5 This can masquerade as ischemic heart disease, despite the absence of any coronary artery atherosclerosis.
We hereby present a case of a 40-year-old female with complaints of chest pain who was brought to the Cardiothoracic Intensive Care Unit (CTVS ICU) when she developed ventricular ectopics and ST segment changes on EKG monitoring. The transesophageal echocardiography (TEE), performed using Philips Epiq 7 (Bothell, WA) X7–2T TEE Probe (2–6 MHz), revealed a large ostium secundum ASD measuring 4.2 cm with left-to-right shunt. The patient had dilated right atrium (RA), right ventricle (RV), left atrium (LA), and pulmonary artery (PA). On midesophageal aortic valve short axis (SA) view (Fig. 1), the LMCA appeared to be significantly narrowed (diameter—0.24 cm). The PA, in the midesophageal ascending aortic SA view (Figs. 2 and 3), was grossly dilated (diameter—3.8 cm), dynamically compressing the LMCA. The dynamic compression is evident in this view, as seen in the video clip (Video 1). The TEE findings were subsequently confirmed using CT angiography, and the patient was planned for ASD closure with coronary artery bypass graft (CABG) surgery. ASD closure using dacron patch and left internal mammary artery to left anterior descending artery graft was performed. Following the surgery, patient was placed on mechanical ventilation in ICU for 8 hours and then successfully extubated with no adverse events.
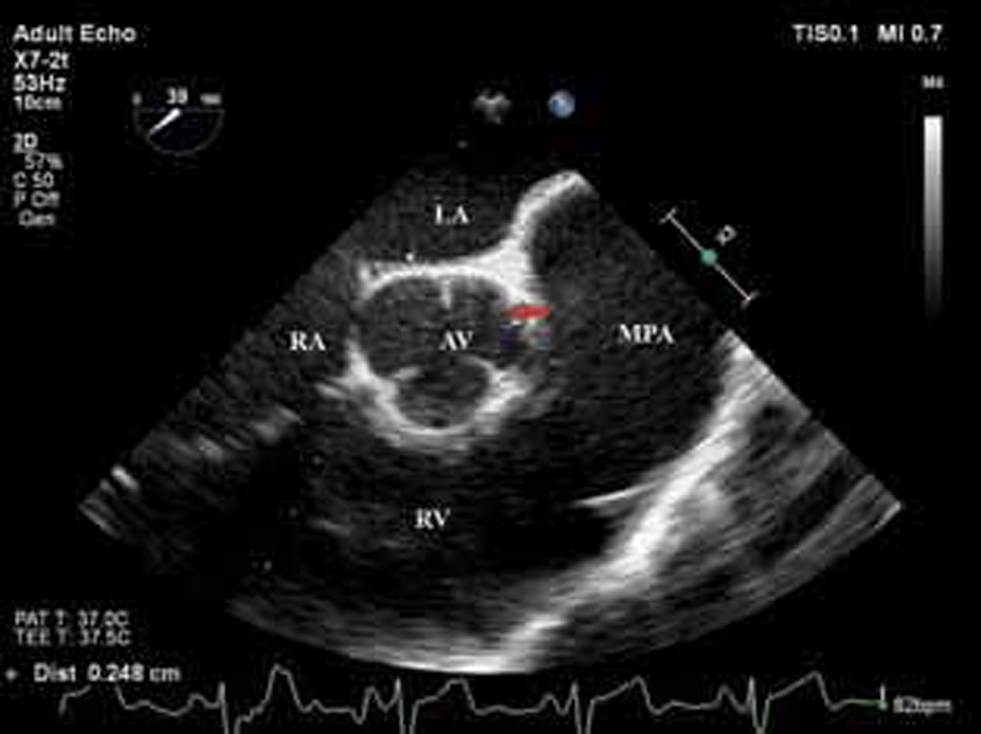
- Two-dimensional transesophageal echocardiography (2D TEE), midesophageal aortic valve short axis (SA) view, showed narrowing of left main coronary artery (LMCA). LA, left atrium; RA, right atrium; AV, aortic valve; RV, right ventricle; MPA, main pulmonary artery.

- Three-dimensional transesophageal echocardiography (3D TEE), midesophageal aortic valve short axis (SA) view, showed left main coronary artery (LMCA) (arrows) located adjacent to the aortic valve (AV) with apparent extraluminal stenosis. RV, right ventricle.
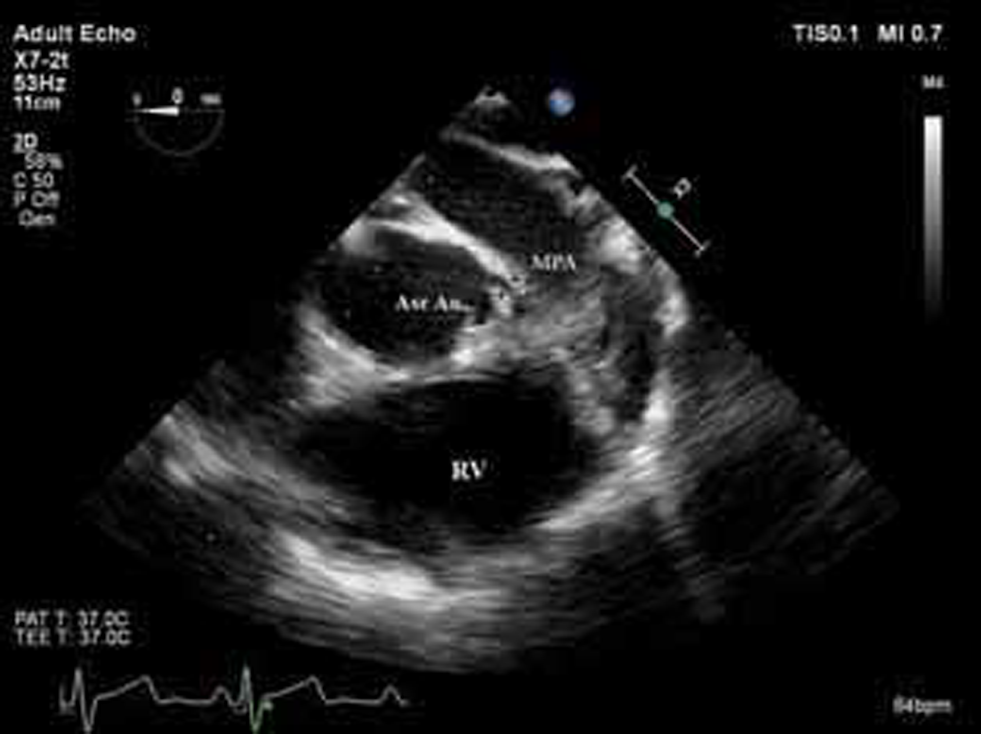
- Two-dimensional transesophageal echocardiography (2D TEE), midesophageal ascending aortic short axis (SA) view, showed left main coronary artery (LMCA) course (arrows) between ascending aorta (Asc Ao) and pulmonary artery (PA). RV, right ventricle; MPA, main pulmonary artery.
Conflict of Interest
We do not have any conflict of interest or any commercial or financial interest in this material. We agree to abide by the rules of your journal regarding publication of this article.
References
- Noninvasive visualization of the left main coronary artery by cross-sectional echocardiography. Circulation. 1976;54(2):169-174.
- [Google Scholar]
- Left main coronary artery extrinsic compression syndrome: a combined intravascular ultrasound and pressure wire. J Invasive Cardiol. 2006;18(3):E102-E104.
- [Google Scholar]
- Left main coronary artery compression in pulmonary hypertension. Catheter Cardiovasc Interv 2020
- [CrossRef] [Google Scholar]
- Pulmonary hypertension causing left main coronary artery compression. Eur Heart J Case Rep. 2020;4(5):1-3.
- [Google Scholar]




