
Translate this page into:
24-Hour Blood Pressure Control with Amlodipine: A Review of the Current Scenario

Kumar Gaurav, MD Dr. Reddy's Laboratories 7-1, 27, Ameerpet Rd, Leelanagar, Ameerpet, Hyderabad, Telangana 500016 India drgauravbhu@gmail.com
This article was originally published by Thieme Medical and Scientific Publishers Pvt. Ltd. and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Introduction Hypertension is the leading cause of cardiovascular diseases and premature death worldwide. Antihypertensive therapy using calcium channel blockers (CCBs) is one of the preferred choices to treat blood pressure (BP) and control blood pressure variability (BPV). In contrast to clinic BP, 24-hour ambulatory BP monitoring (ABPM) has evolved into an accurate and reproducible tool for the assessment and management of hypertension. Amlodipine, a longer acting dihydropyridine CCB is effective for 24 hours BP control and also minimizing BPV. The present article is the comprehensive review highlighting the efficacy of amlodipine in controlling 24-hour BP and minimizing BPV from the review of recent studies.
Materials and Methods The literature search was done using PubMed, Google Scholar, and MEDLINE databases. The studies to be included for review, were identified through the keywords: “amlodipine,” “ambulatory BP monitoring (ABPM),”“blood pressure variability (BPV),” “CCBs,” and filtering articles published in English language only.
Results Pharmacological evidence suggests that amlodipine has the ability to block all the subtypes of CCBs such as L-, N-, P-, Q-, R-, and T-type. Various clinical studies reported that amlodipine is a powerful, well-tolerated, and safe antihypertensive agent which is widely used either alone or as a key component of combination therapy for control of 24 hours BP.
Conclusion Overall, amlodipine is a proven and effective antihypertensive drug and helpful in controlling 24-hour BP, minimizing BP variability and hence reducing the risk of cardiovascular complications.
Keywords
hypertension
amlodipine
calcium channel blockers

Introduction
Hypertension is an important worldwide public-health challenge, often referred to as “the silent killer” owing to it being a major risk for myocardial infarction (MI) and the most important risk factor for stroke.1 Globally, high systolic blood pressure (SBP) is the leading risk factor accounting for 10.4 million deaths and 218 million disability-adjusted life-years (DALYs).2
The World Health Organization (WHO) estimates that of 1.13 billion people with hypertension worldwide, two-thirds are in low and middle income countries (LMICs) and this number is expected to increase over 1.56 billion by 2025. A systematic review and meta-analysis of 242 studies reported that in LMICs, one in three persons had hypertension (mean age: 45.9 ± 12.1 years).3 In India, hypertension is a significant public health problem. A recent national level survey conducted across 24 states and union territories of India reported an overall prevalence of 30.7% in adults, implying that almost one in three participants has hypertension.4 However, only less than one in five people with hypertension have the blood pressure (BP) under control.5, 6 An important reason for poor BP control may be late or ineffective treatment that could lead to irreversible or difficult to reverse adaptations of the cardiovascular (CV) system.7 Trials like Valsartan Antihypertensive Long term Use Evaluation (VALUE), the Study on Cognition and Prognosis in the Elderly (SCOPE), and the Systolic Hypertension in Europe (Syst-Eur) trials suggested the importance of early and 24-hour control of BP with regards to CV outcome (Fig. 1).8
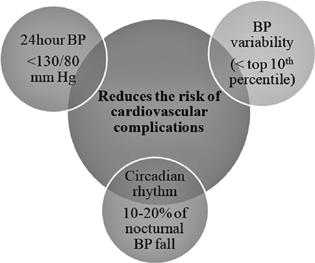
- Relation between 24-hour BP control and cardiovascular complications.
It has been long recognized that BP varies as per circadian rhythm, dipping at night during rest, increasing steeply in the morning (known as the “morning surge”), and peaking typically in the late afternoon.9 Thus, measurement of blood pressure variability (BPV) over a period of 24 hours (outside clinic) is recommended. The 24-hour readings obtained during the patient's daily activities provide a precise assessment of the true BP. The main prognostic features of 24-hour BP measurement are daytime ambulatory systolic/diastolic BP, night time ambulatory SBP, night time ambulatory diastolic BP, ambulatory pulse pressure, and presence or absence of nocturnal dip. Ambulatory blood pressure monitoring (ABPM) is now considered better in diagnosing hypertension outside of a clinic environment10, 11, 12 as BP is measured at daytime and night time at different intervals. Majorly, ABPM includes repeated measurement of BP at predetermined intervals ranging from 10 to 60 minutes during the day and night time. A previously published study concluded that ABPM gave the most accurate measurement of BP in comparison to home or clinical measurements.13
Further, ABPM can measure the BPV and eliminates observer bias.
Recent studies also suggested shortcomings in the measurement of office BP related to device, observer, and patient-related factors. White coat hypertension is a commonly encountered phenomenon wherein, a higher BP reading is observed at doctor's office. Masked hypertension and nocturnal hypertension are also not diagnosed with office BP.14 Based on these observations, the hypertension guidelines are continually evolving, translating new knowledge to clinical practice.15 Earlier, the guidelines were more focused on absolute decrease in SBP/DBP but a paradigm shift to monitor 24-hour BP obtained during the patient's daily activities for a precise assessment of the true BP was incorporated in all the hypertension guidelines.16 Further, ABPM has been recognized as a better predictor of clinical outcomes in numerous studies.17, 18, 19 A study conducted in 1,007 subjects showed that 24-hour daytime and night time AMBPs were closely associated with the risk of silent cerebrovascular lesions detected by brain magnetic resonance imaging, whereas the clinic BP values were not associated with subclinical cerebrovascular events.20 The Syst-Eur Trial sub-study also noted that in elderly subjects with untreated isolated systolic HTN, ABPM was a significant predictor of CV risk.21 A systematic review of 20 studies concluded that ABPM gave the most accurate measurement of BP in comparison to home or clinic measurements.22 The threshold values for ABPM in guidelines NICE, JNC-8, ESH/ESC/ are summarized in Table 1.
|
Organization, year |
Indications |
Diagnostic protocol and threshold |
Ambulatory blood pressure monitoring, mm Hg |
|---|---|---|---|
|
American Society of Hypertension, 201455 |
Hypertension, white-coat hypertension |
Diagnosis confirmed: at an additional patient visit, usually 1–4 wk after the first measurements. OBPM diagnostic threshold: ≥140/90 mm Hg HBPM diagnostic threshold: ≥135/85 mm Hg |
ABPM is another approach if available. |
|
Joint National Committee on Prevention, Detection, Evaluation and Treatment of Blood Pressure (JNC 7), 200456 |
Suspected white-coat hypertension among hypertensive patients and no target organ damage; hypotensive symptoms with antihypertensive medication |
Stage 1 hypertension diagnosis should be confirmed within 2 mo after initial elevated OBPM (no further protocol details reported). Stage 2 hypertension should be confirmed within 1 mo; those with ≥180/110 mm Hg evaluate and treat immediately. |
ABPM diagnostic threshold: ≥135/85 (awake), ≥120/75 (asleep) |
|
National Institute for Health and Care Excellence, 201157 |
Hypertension, white-coat hypertension |
Adults aged 18–21 y only. Based on repeated measures in both arms followed by ABPM (at least 14 measurements) or HBPM (twice in morning and evening for at least 4 d, ideally 7 d) if ABPM not tolerable. OBPM diagnostic threshold: ≥140/90 mm Hg |
ABPM diagnostic threshold: ≥135/85 (daytime) |
|
National Heart, Lung, and Blood Institute, 201358 |
Hypertension, white-coat hypertension |
Based on two OBPM measurements, confirm elevated reading with contralateral arm. |
|
|
University of Michigan Health System, 200955 |
Hypertension, white-coat and masked hypertension |
Based on taking mean blood pressure levels from recordings over several visits. Suspected white-coat hypertension: three or more OBPM >140/90 mm Hg |
ABPM <140/90 |
|
Canadian Hypertension Education Program (CHEP), 201359 |
Hypertension, suspected white-coat hypertension, and masked hypertension |
OBPM diagnostic threshold: ≥160/110 mm Hg averaged across three visits; or if ≥140/90 mm Hg averaged across five visits |
ABPM diagnostic threshold: ≥135/85 (awake) or ≥130/80 (24 hours) HBPM diagnostic threshold: ≥135/85 |
|
European Society of Hypertension, 200860 |
Sustained, masked or white-coat hypertension |
HBPM diagnostic threshold: 135/85 mm Hg |
ABPM diagnostic threshold: ≥135/85 (awake), ≥120/70 (asleep) and ≥130/80 (24 h) |
|
Institute for Clinical Systems Improvement, 201261 |
Confirming initial elevated BP; white-coat or masked hypertension |
Based on a combination of one or more follow-up visits with at least two blood pressure readings at each visit and an out-of-office blood pressure measurement (e.g., HBPM) or 24 h ABPM. |
ABPM diagnostic threshold: 140/85 (awake), 120/70 (asleep), and 130/80 (24 h) |
|
HOPE ASIA 2020 Guidelines |
ABPM: gold standard for diagnosing and monitoring of hypertension |
Diagnostic thresholds for hypertension using ABPM are as follows: average 24-h BP of ≥130/80 mm Hg; average daytime BP of ≥135/85 mm Hg |
|
|
ISH 2020 Guidelines |
Confirming initial elevated BP; white-coat or masked hypertension |
ABPM: 24-h average ≥130 and/or ≥80, Day time (or awake) average ≥135 and/or ≥85, Night time (or asleep) average ≥120 and/or ≥70, HBPM ≥135 and/or ≥85 |
|
|
Japanese Society of Hypertension, 200962 |
Diagnosis of essential, white-coat, and masked hypertension |
Based on blood pressures measured on at least two different clinic-based occasions. OBPM diagnostic threshold: ≥140/90 mm Hg HBPM diagnostic threshold: ≥135/85 mm Hg |
ABPM diagnostic threshold: ≥130/80 (24 hour), ≥135/85 (day), ≥120/70 (night) |
|
Comparison of National recommendations for Ambulatory BP (Clinic BP = 140/90 mm Hg) |
|||
|
Guideline |
Ambulatory BP monitoring mm Hg |
||
|
24 h |
Night |
Day |
|
|
Seventh Joint National Committee (USA, 2003)63 |
Not stated |
120/75 |
135/85 |
|
European Society of Hypertension (2013)64 |
130/80 |
120/70 |
135/85 |
|
Japanese Circulation Society (2012)65 |
130/80 |
120/70 |
135/85 |
|
Canadian Hypertension Society (1999)66 |
130/80 |
120/75 |
135/85 |
|
Australian National Heart Foundation and High BP Research Council Consensus (2012)67 |
130/80 |
120/75 |
135/85 |
|
National Institute for Health and Clinical Excellence (UK, 2011)40 |
Not stated |
Not stated |
135/85 |
Abbreviations: HBPM, home blood pressure monitoring; NR, not reported; OBPM, office blood pressure measurement.
A substantial number of studies advocated that BPV (ultrashort term, short term and long term) is a causative factor for different CV diseases like left ventricular hypertrophy (LVH) that further leads to organ damage.23 BPV or the fluctuation in the BP is complex and includes both the short-term (within minutes to hours) and long-term variations (includes days and months); the latter being more reliable than former on the grounds that it is better predictor of the CV outcomes.24 Accordingly, CV protection by antihypertensive treatment should aim not only at achieving control of the average BP values, but also at stabilizing BPV. The ability of ABPM to provide a quantification of BP throughout the 24-hour period during an individual's normal daily routine is one of the reasons for its high prognostic value.
To avoid the risk of CV complications, it is crucial that the 24-hour BPV is controlled. Thus, an antihypertensive drug with low BPV and a high smoothness index (SI) is a pragmatic approach. SI provides a useful measure of antihypertensive treatment efficacy over the 24-hour dosing period, its values being highest with antihypertensive agents that have large and consistent effects across 24 hours. A large SI usually indicates a consistent average BP reduction associated with a small variability among hours, and thus a superior CV protection and an improved prevention of target-organ damage.25 An ideal anti-hypertensive therapy, thus, has a multi-modal approach; it should have a longer half-life, should be able to control BP over a period of 24 hours, should be able to reduce BPV, and should have a higher SI.
Amlodipine for the Management of Hypertension
All the major hypertensive guidelines recommend calcium channel blockers (CCBs) as one of the first line antihypertensive drugs. Trials like ALLHAT, VALUE, ASCOT, and ACCOMPLISH recommend CCB-based therapy for the management of normal and high CV risk hypertensive patients.
Amlodipine, a long-acting, lipophilic, third generation dihydropyridine (DHP) CCB has demonstrated a strong evidence of safety and efficacy in BP and CV event reduction in large randomized controlled trials. The outcomes of these trials are summarized in Table 2. The WHO has mentioned amlodipine in its list of essential medicines and it is denoted as the safest and most effective medicine required in health system.13
|
Trial (Experiment vs. control) |
No of patients |
Follow up (Years) |
Outcome of interest (No of events) |
Survival analysis [(OD/HR/RR) 95% CI] |
||||
|---|---|---|---|---|---|---|---|---|
|
Fatal CHD/MI |
Stroke |
All-cause mortality |
CHD |
Stroke |
All-cause mortality |
|||
|
VARTc (Amlodipine vs. Valsartan) |
Amlodipine:316 |
3.4 |
1 |
7 |
2 |
1.04 (0.07–16.5) |
1.18 (0.43–3.23) |
0.69 (0.12–4.1) |
|
Valsartan: 305 |
1 |
8 |
3 |
|||||
|
ALLHATa (Amlodipine vs. Lisinopril) |
Amlodipine: 9,048 |
4.9 |
798 |
377 |
1256 |
1.01 (0.91–1.11) |
1.05 (0.97–1.13) |
1.23 (1.08–1.41) |
|
Lisinopril: 9,054 |
796 |
457 |
1354 |
|||||
|
CAMELOTb (Amlodipine vs. Enalapril) |
Amlodipine: 673 |
2 |
110 |
6 |
7 |
0.69 (0.54–0.88) |
0.50 (0.19–1.32) |
0.92 (0.33–2.52) |
|
Enalapril: 663 |
136 |
12 |
6 |
|||||
|
ASCOT (Amlodipine vs. Atenolol) |
Amlodipine: 2,565 |
5.5 |
93 |
18 |
245 |
0.89 (0.67–1.17) |
0.82 (0.44–1.52) |
0.98 (0.82–1.17) |
|
Atenolol: 2,572 |
105 |
22 |
250 |
|||||
|
VALUEc (Amlodipine vs. Valsartan) |
Amlodipine: 7,596 |
4.2 |
313 |
281 |
818 |
1.19 (1.02–1.38) |
1.15 (0.98–1.35) |
1.04 (0.94–1.14) |
|
Valsartan: 7,649 |
369 |
322 |
841 |
|||||
Abbreviations: ALLHAT, The Antihypertensive and Lipid-Lowering Treatment to Prevent Heart Attack Trial; ASCOT, Anglo-Scandinavian Cardiac Outcomes; CAMELOT, The Comparison of Amlodipine vs Enalapril to Limit Occurrences of Thrombosis; CHD, coronary heart disease; CI, confidence interval; HR, hazard ratio; MI, myocardial infarction; OD, odds ratio; RR, relative risk; VALUE, The Valsartan Antihypertensive Long-term Use Evaluation; VART; Valsartan Amlodipine Randomized Trial.
Amlodipine: Blocks All Types of Calcium Channels
Broadly, CCBs reduce the influx of calcium ions into the vascular and cardiac smooth muscle cells which help in pumping of blood smoothly by heart. Calcium channels (Ca2+) are broadly classified into at least six subtypes; namely, L-, N-, P-, Q-, R-, and T-type, based on electrophysiological and pharmacological evidence. L-type of voltage-gated CCBs are used as a first or second line drug in the management of hypertension as they are potent vasodilators. Amlodipine confers the pharmacological action by inhibiting the voltage-gated calcium ion channel (CaV).26 The L-type calcium channel is inhibited by amlodipine that prevents the influx of calcium ions into the transmembrane of cardiac and vascular smooth muscle cell.27 Amlodipine is not only an L-type but also an N-type and P/Q-type CCBs as published studies reported that amlodipine blocks N-type Ca2+ and P/Q-type channels as well. Furthermore, the kinetic interaction of amlodipine shows a very slow rate of association and dissociation from its binding sites that lead to a gradual onset of action(Fig. 2).28
Pharmacological Actions Evidencing Clinical Efficacy
The elimination of amlodipine from the plasma is biphasic and the termination half-life is approximately 30 to 50 hours. The renal route is the preferred route of excretion of metabolites of amlodipine; however, a part (20–25%) is also excreted via biliary route.
Effect on Blood Pressure and Other Hemodynamic Effects
A summary of all the clinical studies targeting the efficacy of amlodipine in reducing BP is represented in Table 3. Amlodipine at a mean dose of 10 mg effectively controlled BP throughout the 24 hours both at rest and during the exercise by lowering the total peripheral resistance without lowering the cardiac output.29
|
Primary citation of study |
Design of study |
Dosea |
Study duration |
Primary end point of interest |
Resultb |
|---|---|---|---|---|---|
|
Silke et al68 |
Treatment versus no treatment control group |
20 mg (IV) amlodipine |
Immediate dose response was measured |
Mean reduction in SBP and DBP |
Control (SBP/DBP): 145 ± 5/130 ± 4 mm Hg; Treatment (SBP/DBP): 80 ± 2/72 ± 2 mm Hg |
|
Lund-Johansen et al29 |
Placebo-controlled |
Amlodipine 5 mg initially and 10 mg (if necessary) |
11 mo |
Mean reduction in BP at rest (sitting) and after work (sitting) |
Rest: Placebo group; 182 ± 16.1 (SBP)/111.2 ± 8.1 mm Hg (DBP); After treatment at rest; 153.4 ± 10.7/95.6 ± 5.7 mm Hg (SBP/DBP) After work (without treatment); 204 ± 12.9/112.7 ± 8.1 mm Hg; After treatment: 176.9 ± 15.5 (SBP)/96.9 ± 7.9 (DBP) mm Hg |
|
Broadhurst et al69 |
Placebo-controlled |
5 mg (2 wk) amlodipine initially and thereafter 10 mg (4 wk) |
6 wk |
Reduction in mean supine cuff BP |
Placebo group: 169/104 mm Hg Treatment group: 146/92 mm Hg |
|
Burris et al33 |
Double-blind, randomized placebo-controlled, and single-site |
5 mg amlodipine |
4 wk |
Mean reduction in supine BP from baseline |
Baseline (SBP/DBP to final (SBP/DBP); Placebo: 146.9/100 to 154 mm Hg/97.3 mm Hg; Treatment: 156/99.3 to 138/86.3 mm Hg |
|
Sharma et al41 |
Comparative, phase-3, multicenter, and prospective |
5 mg (amlodipine), and telmisartan 40 mg + amlodipine 5 mg (FDC) |
12 wk |
Reduction in SBP and DBP |
SBP: A [16.6%], (T + A [−27.4%]; DBP: (T + A [20.1%]; A [−13.3%]) (all, p <0.05) |
|
Bahl et al70 |
Prospective and multicenter |
FDC (perindopril; 4 mg and amlodipine 5 mg) |
60 d |
Mean change in BP from baseline |
−41.9 ± 34.8 (SBP)/− 23.2 ± 21.8 (DBP) mm Hg; p <0.0001) from baseline (167.4 ± 15.2/101.4 ± 9.1 mm Hg) |
|
El-Etriby et al71 |
Multicenter, open label, prospective, and cohort |
SPC: Aml/Val/HCTZ; 10/160/25 mg or 5/160/12.5 mg |
12 wk |
Mean change in BP from baseline |
165.5 ± 12.83/100.8 ± 7.03 mm Hg from baseline (129.7 ± 8.35/80.6 ± 5.25 mm Hg); (p < 0.0001) |
|
Dharapurand Patil72 |
Parallel group, open label, prospective, and comparative |
Amlodipine (5–10 mg) |
8 wk |
Mean change in BP from baseline |
SBP: 132.72 ± 4.91 mm Hg; DBP: 82 ± 2.55 from baseline (151.56 ± 10.21/95.4 ± 5.70 mm Hg) |
|
Nwachukwu et al73 |
Single-blind randomized |
Amlodipine 5 mg |
4 wk |
Reduction in SBP and DBP |
SBP: −17.69 ± 3.12 mm Hg; DBP: −12.36 ± 2.40 mm Hg |
Abbreviations: Aml, amlodipine; BP, blood pressure; DBP, diastolic blood pressure; FDC, fixed dose combination; HCTZ, hydrochlorothiazide; IV, intravenous; SBP, systolic blood pressure; SPC, single pill combination; Val, valsartan.
Evidence of 24 Hours BP Control by Amlodipine
Compared with nifedipine and other medications in the DHP class, amlodipine has the longest half-life at 30 to 50 hours; longer half-life confers it the ability to have once daily dosing (Table 4).
Amlodipine shows a gradual and prolonged reduction in BP due to its longest elimination half-life and slow receptor dissociation kinetics. Zhang et al conducted a X-CELLENT trial with 577 patients and reported that amlodipine was efficacious and tolerable across all timeframes even after adjustment for mean BP reduction as it significantly decreased daytime, night time and 24-hour SBP variability; whereas indapamide significantly decreased SBP variability in the daytime and 24 hours.30 The Circadian Anti-Ischemia Program in Europe (CAPE), a large, 10-week international (63 sites), double-blind, parallel study conducted with 1160 patients reported that amlodipine significantly reduced both symptomatic and asymptomatic ischemic events over 24 hours in patients with chronic stable angina.31 Another pooled analysis of five different studies reported that BPV with amlodipine was significantly (p <0.0001) lower compared with atenolol, lisinopril, and enalapril.32 A randomized trial reported that amlodipine 5 mg once daily, was well tolerated and effective in maintaining both DBP and SBP below the baseline levels at every hour during the 24-hour observation period.33 A comparative analysis of valsartan and hydrochlorothiazide and amlodipine reported that amlodipine was as effective as valsartan and hydrochlorothiazide in controlling the 24-hour BP as well as night time and daytime BP levels from baseline.34
A considerable number of studies estimated the efficacy of amlodipine on ABPM through a reliable parameter; SI whose higher value indicates a better antihypertensive effect. SI is calculated as the ratio between the average of the 24 hourly BP changes induced by a given medication and the standard deviation of hourly reductions and it represents the useful measures of the homogeneity of the antihypertensive effect over 24 hours; in fact the SI provides a superior measure of the homogeneity of BP.35 All combination therapies have higher SI than monotherapy. Amlodipine is consistent in BP reduction throughout 24 hours because of a high trough to peak concentration (T: p = 0.85) and a high SI. The 24-hour SI value for amlodipine 5 mg was higher than those of manidipine, lercanidipine, nifedipine, felodipine, and diltiazem.25 A meta-analysis of 11 randomized studies encompassing 5,188 hypertensive patients that investigated the SI of losartan, valsartan, telmisartan, ramipril, and amlodipine, reported that amlodipine 5 mg had higher SI than any other anti-hypertensive agent. In the same study, amlodipine 5 mg was found to have a higher SI than lercanidipine and manidipine in the patients with mild to moderate hypertension.36 Amongst spirapril and amlodipine, SI of amlodipine (0.65/0.45) was reported to be higher (spirapril: 0.55/0.45) implying high advantages for amlodipine in the long-term treatment.37 Cho et al in their 20-week study reported that 24-hour ambulatory central BP was well controlled in losartan/amlodipine (−9.7 ± 10.67 mm Hg) group as compared with losartan/HCZ (−6.28 ± 10.50 mm Hg) group. Moreover, the pulse pressure was also significantly reduced in the amlodipine (45.4 ± 8.1 mm Hg) group than that (48 ± 8.3 mm Hg) in the HCZ group.38 Huang et al reported that amlodipine was more efficacious (2–3 mm Hg) than nifedipine in reducing the 24-hour BP when the dose of medication got missed.39 A phase IV study investigated the effect of amlodipine/valsartan on the mean 24-hour ambulatory BP when given in the morning (6–10 am) and evening (6–10 pm). Following 4 weeks of treatment, the patients who took dose in morning, and evening showed a mean reduction of −12.16 (0.88)/− 11.17 (0.90) mm Hg in SBP, respectively while the reduction of DBP in morning, and evening was −7.71 (0.59) and −7.01 (0.60) mm Hg, respectively.40 A study reported that amlodipine in combination with either perindopril or HCZ was more effective at reducing ABPM as compared with the FDC of HCZ/perindopril in Black African patients. The mean difference in 24-hour SBP between baseline and following 6 months of amlodipine/HCZ and amlodipine/perindopril therapy was −3.14 and −3 mm Hg, respectively that were comparable to the mean reduction of −2.59 mm Hg in HCZ/perindopril group.41
Outcome Benefits of Amlodipine in Cardiovascular Diseases and Renal Failure
LVH generally develops in response to hypertension and causes left ventricle to work harder.42 Antihypertensive drugs are known to lower the risk of LVH by maintaining the BP within range. Long-acting CCB administration is helpful in maintaining the serial changes in left ventricular (LV) function and morphology in hypertensive patients with LV hypertrophy. A study of 32 hypertensive patients demonstrated that administration of 5 mg amlodipine/d resulted in a significant decrease in SBP within 1 month and a significant reduction in septal thickness and LV mass index at 6 and 12 months.17 Yilmaz et al in a study with 112 hemodialysis patients observed that LV mass index decreased in subjects with concentric LVH after administration of amlodipine.18 Another study conducted by Adalet et al also reported similar results in 19 patients with hypertension; amlodipine was effective in lowering the BP and reduced the risk for LVH in all the patients.43
Some major trials reported promising effects of amlodipine on varied CV diseases. Prospective Randomized Amlodipine Survival Evaluation Study Group (PRAISE) reported that amlodipine improved the morbidity and mortality in the patients with non-ischemic cardiomyopathy, but not the ones with ischemic heart diseases.44 In the PREVENT study, amlodipine retarded the progress of coronary atherosclerosis, and incidence of CV events was not increased.45 The VALUE study demonstrated that there is no difference in the incidence of heart failure or stroke between amlodipine- and valsartan-treated patients, in fact the incidence of MI was rather lower in amlodipine-treated group.46 Amlodipine is also demonstrated to reduce CV events compared with enalapril and placebo in the CAMELOT study.47
Another public health problem associated with hypertension is altered urinary albumin creatinine ratio which is an early sign of kidney damage. Microalbuminuria in hypertensive patients is associated with increased mortality and it is an independent risk factor for CV and cerebrovascular complications.5 A randomized trial conducted with 72 patients with hypertension and type 2 diabetes mellitus reported that CCBs can help in the reduction of microalbuminuria as CCBs dilate afferent arterioles and possibly increase intraglomerular pressure. They found that anti-albuminuric effect of cilnidipine is similar to anti-albuminuric effect of amlodipine.48
Effect on Kidney
The beneficial pharmacological effects of amlodipine on kidney have been very well documented in preclinical and clinical studies and discussing all of them will be out of scope of this review. An interesting fact about these studies is that they advocate the counteracting effect conferred by amlodipine on the norepinephrine, angiotensin II, and dilatation of afferent and efferent arteriole that are increased in the patient with hypertension. Amlodipine was reported to lower the mean arterial pressure along with the increase in the value of p-aminohippurate clearance (19%), inulin clearance (13%), and a decrease in renal vascular resistance (25%) in the patients with hypertension.49 In a 1 year study comparing amlodipine with enalapril, an annual decline in creatinine clearance was reported to be −3.7 mL/min/y and −2.6 mL/min/y in amlodipine and enalapril group, respectively in hypertensive patients with renal abnormalities.50
Cost-Effectiveness of Amlodipine-Based Treatment Regimen
The cost of antihypertensive drugs imposes a huge burden on patients. A study conducted by Chan et al reported that amlodipine-based treatment regimen has not only better effectiveness but is also predicted to be cost saving when compared with valsartan.51 Studies conducted in Europe, North America, and China showed that amlodipine was associated with improved clinical outcomes and lower total cost compared with traditional treatments for hypertension or coronary artery disease.52, 53
In India, cost effectiveness analysis of antihypertensive drugs reported atenolol to be the most cost-effective drug (INR 5.5/unit of effectiveness), followed by the amlodipine and losartan combination (INR 5.6) and amlodipine (INR 6.3).54
Conclusion
Amlodipine is a trusted and well-tested CCB that blocks all the subtypes of calcium channels, effectively controls BP while maintaining circadian rhythm and reduces the risk of CV and cerebrovascular complications. Amlodipine is an excellent first line choice among all the other antihypertensive agents. The efficacy and safety of amlodipine are extensively studied and well established as a monotherapy as well as a combination therapy. Amlodipine with an effective BP control over 24 hours and low BPV reduces the progression of severe complications. Its longer half-life and higher SI lead to a consistent average BP reduction. Amlodipine is a trusted and cost-effective option not only for controlling BP but also for safely improving patient outcomes.
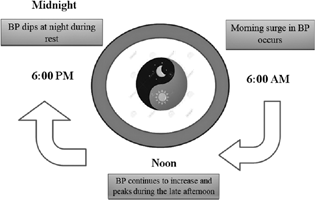
- Circadian rhythm
Acknowledgment
The authors acknowledge the Knowledge Isotopes Pvt. Ltd (www.knowledgeisotopes.com) for medical writing support.
Conflict of Interest
K.G. and S.S. are employees of Dr. Reddy's Laboratories. T.N., A.S.K., T.G.U. and M.H.T. are advisory board members for Dr. Reddy's Laboratories.
Funding None.
References
- Global, regional, and national comparative risk assessment of 84 behavioural, environmental and occupational, and metabolic risks or clusters of risks, 1990-2016: a systematic analysis for the Global Burden of Disease Study 2016. Lancet. 2017;390:1345-1422. (10100):
- [Google Scholar]
- Prevalence of hypertension in low-and middle-income countries: a systematic review and meta-analysis. Medicine (Baltimore). 2015;94(50):e1959.
- [Google Scholar]
- Prevalence of hypertension among Indian adults: Results from the great India blood pressure survey. Indian Heart J. 2019;71(4):309-313.
- [Google Scholar]
- Prevalence and association of microalbuminuria in essential hypertensive patients. N Am J Med Sci. 2012;4(8):331-335.
- [Google Scholar]
- Achievement of treatment goals for primary prevention of cardiovascular disease in clinical practice across Europe: the EURIKA study. Eur Heart J. 2011;32(17):2143-2152.
- [Google Scholar]
- Is early and fast blood pressure control important in hypertension management? Int J Cardiol. 2018;254:328-332.
- [Google Scholar]
- The importance of early antihypertensive efficacy: the role of angiotensin II receptor blocker therapy. J Hum Hypertens. 2006;20(3):169-175.
- [Google Scholar]
- Circadian clock-mediated regulation of blood pressure. Free Radic Biol Med. 2018;119:108-114.
- [Google Scholar]
- New Algorithm for the Diagnosis of Hypertension: Canadian Hypertension Education Program Recommendations. Oxford University Press; 2005.
- [Google Scholar]
- Home measurement of blood pressure and cardiovascular disease: systematic review and meta-analysis of prospective studies. J Hypertens. 2012;30(3):449-456.
- [Google Scholar]
- Home-measured blood pressure is a stronger predictor of cardiovascular risk than office blood pressure: the Finn-Home study. Hypertension. 2010;55(6):1346-1351.
- [Google Scholar]
- Efficacy of a Combination of Amlodipine/Valsartan on 24H Blood Pressure Control With One Nocturnal or Diurnal Intake a Day. Accessed on June 04, 2020 at:
- [Publisher] [Google Scholar]
- The rational clinical examination. Does this patient have hypertension? How to measure blood pressure. JAMA. 1995;273(15):1211-1218.
- [Google Scholar]
- Assessment and management of blood-pressure variability. Nat Rev Cardiol. 2013;10(3):143-155.
- [Google Scholar]
- Impact of azelnidipine and amlodipine on left ventricular mass and longitudinal function in hypertensive patients with left ventricular hypertrophy. Echocardiography. 2014;31(10):1230-1238.
- [Google Scholar]
- Impact of amlodipine or ramipril treatment on left ventricular mass and carotid intima-media thickness in nondiabetic hemodialysis patients. Ren Fail. 2010;32(8):903-912.
- [Google Scholar]
- Ambulatory blood pressure monitoring predicts cardiovascular events in treated hypertensive patients–an Anglo-Scandinavian cardiac outcomes trial substudy. J Hypertens. 2009;27(4):876-885.
- [Google Scholar]
- Ambulatory versus home versus clinic blood pressure: the association with subclinical cerebrovascular diseases: the Ohasama Study. Hypertension. 2012;59(1):22-28.
- [Google Scholar]
- Predicting cardiovascular risk using conventional vs ambulatory blood pressure in older patients with systolic hypertension. JAMA. 1999;282(6):539-546.
- [Google Scholar]
- Relative effectiveness of clinic and home blood pressure monitoring compared with ambulatory blood pressure monitoring in diagnosis of hypertension: systematic review. BMJ. 2011;342:d3621.
- [Google Scholar]
- Blood pressure variability, cardiovascular risk, and risk for renal disease progression. Curr Hypertens Rep. 2012;14(5):421-431.
- [Google Scholar]
- Blood pressure variability: prognostic value and therapeutic implications. ISRN hypertension.
- [Google Scholar]
- Blood pressure variability over 24 h: prognostic implications and treatment perspectives. An assessment using the smoothness index with telmisartan-amlodipine monotherapy and combination. Hypertens Res. 2014;37(3):187-193.
- [Google Scholar]
- Amlodipine in hypertension: a first-line agent with efficacy for improving blood pressure and patient outcomes. Open Heart. 2016;3(2):e000473.
- [Google Scholar]
- Discovery and development of calcium channel blockers. Front Pharmacol. 2017;8:286.
- [Google Scholar]
- Long-term haemodynamic effects of amlodipine at rest and during exercise in essential hypertension. Cardiology. 1992;80(01):37-45.
- [Google Scholar]
- Effect of antihypertensive agents on blood pressure variability: the Natrilix SR versus candesartan and amlodipine in the reduction of systolic blood pressure in hypertensive patients (X-CELLENT) study. Hypertension. 2011;58(2):155-160.
- [Google Scholar]
- Amlodipine reduces transient myocardial ischemia in patients with coronary artery disease: double-blind Circadian Anti-Ischemia Program in Europe (CAPE Trial) J Am Coll Cardiol. 1994;24(6):1460-1467.
- [Google Scholar]
- Effects of amlodipine and other classes of antihypertensive drugs on long-term blood pressure variability: evidence from randomized controlled trials. J Am Soc Hypertens. 2014;8(5):340-349.
- [Google Scholar]
- The effect of amlodipine on ambulatory blood pressure in hypertensive patients. Am J Cardiol. 1994;73(3):39A-43A.
- [Google Scholar]
- 24-Hour ambulatory blood pressure control with triple-therapy amlodipine, valsartan and hydrochlorothiazide in patients with moderate to severe hypertension. J Hum Hypertens. 2011;25(10):615-622.
- [Google Scholar]
- The smoothness index: an ‘all purposes’ approach to the assessment of the homogeneity of 24-h blood pressure control? J Hypertens. 2019;37(12):2341-2344.
- [Google Scholar]
- Evaluating 24-h antihypertensive efficacy by the smoothness index: a meta-analysis of an ambulatory blood pressure monitoring database. J Hypertens. 2010;28(11):2177-2183.
- [Google Scholar]
- Assessment of amlodipine antihypertensive effect homogeneity in controlled trial. Ration Pharmacother Cardiol. 2009;5(2):22-26.
- [Google Scholar]
- Comparison of 24-hour ambulatory central blood pressure reduction efficacy between fixed amlodipine or up-titrated hydrochlorothiazide plus losartan: the K-central study. Am J Hypertens. 2019;32(10):992-1002.
- [Google Scholar]
- A randomized controlled trial on the blood pressure-lowering effect of amlodipine and nifedipine-GITS in sustained hypertension. J Clin Hypertens (Greenwich). 2019;21(5):648-657.
- [Google Scholar]
- Developing hypertension guidelines: an evolving process. Am J Hypertens. 2014;27(6):765-772.
- [Google Scholar]
- Results of a comparative, phase III, 12-week, multicenter, prospective, randomized, double-blind assessment of the efficacy and tolerability of a fixed-dose combination of telmisartan and amlodipine versus amlodipine monotherapy in Indian adults with stage II hypertension. Clin Ther. 2007;29(12):2667-2676.
- [Google Scholar]
- The effect of amlodipine on the mass and functions of the left ventricle in patients with primary hypertension and left ventricular hypertrophy. Curr Ther Res Clin Exp. 1995;56(6):607-616.
- [Google Scholar]
- Effect of amlodipine on morbidity and mortality in severe chronic heart failure. N Engl J Med. 1996;335(15):1107-1114.
- [Google Scholar]
- Effect of amlodipine on the progression of atherosclerosis and the occurrence of clinical events. Circulation. 2000;102(13):1503-1510.
- [Google Scholar]
- Blood pressure dependent and independent effects of antihypertensive treatment on clinical events in the VALUE Trial. Lancet. 2004;363:2049-2051. (9426):
- [Google Scholar]
- Effect of antihypertensive agents on cardiovascular events in patients with coronary disease and normal blood pressure: the CAMELOT study: a randomized controlled trial. JAMA. 2004;292(18):2217-2225.
- [Google Scholar]
- Reduction in microalbuminuria by calcium channel blockers in patients with type 2 diabetes mellitus and hypertension-a randomized, open-label, active-controlled, superiority, parallel-group clinical trial. Int J Clin Pract. 2017;71(9):e12987.
- [Google Scholar]
- Amlodipine therapy corrects renal abnormalities encountered in the hypertensive state. Am J Kidney Dis. 1987;10(6):446-451.
- [Google Scholar]
- Amlodipine is comparable to angiotensin-converting enzyme inhibitor for long-term renoprotection in hypertensive patients with renal dysfunction: a one-year, prospective, randomized study. Am J Hypertens. 2000;13(9):980-985.
- [Google Scholar]
- Cost-effectiveness of amlodipine compared with valsartan in preventing stroke and myocardial infarction among hypertensive patients in Taiwan. Int J Gen Med. 2016;9:175-182.
- [Google Scholar]
- A cost-effectiveness analysis between amlodipine and angiotensin ii receptor blockers in stroke and myocardial infarction prevention among hypertension patients in China. Value Health Reg Issues. 2013;2(1):75-80.
- [Google Scholar]
- Cost-effectiveness study of antihypertensive drugs in Mumbai, India. Int J Life Sci Pharma Res. 2018;8(1):97-103.
- [Google Scholar]
- Clinical practice guidelines for the management of hypertension in the community: a statement by the American Society of Hypertension and the International Society of Hypertension. J Clin Hypertens (Greenwich). 2014;16(1):14-26.
- [Google Scholar]
- Clinical effectiveness and safety of low cost versus innovator brand amlodipine in hypertension: a single-blinded, randomized, crossover, noninferiority trial. Indian J Pharmacol. 2016;48(6):706-709.
- [Google Scholar]
- Improving quality of life in hypertension management using a fixed-dose combination of olmesartan and amlodipine in primary care. Expert Opin Pharmacother. 2010;11(17):2779-2790.
- [Google Scholar]
- Health-related quality of life impact of a triple combination of olmesartan medoxomil, amlodipine besylate and hydrochlorotiazide in subjects with hypertension. Health Qual Life Outcomes. 2015;13(1):24.
- [Google Scholar]
- The 2014 Canadian Hypertension Education Program recommendations for blood pressure measurement, diagnosis, assessment of risk, prevention, and treatment of hypertension. Can J Cardiol. 2014;30(5):485-501.
- [Google Scholar]
- European Society of Hypertension guidelines for blood pressure monitoring at home: a summary report of the Second International Consensus Conference on Home Blood Pressure Monitoring. J Hypertens. 2008;26(8):1505-1526.
- [Google Scholar]
- The Japanese Society of Hypertension guidelines for the management of hypertension (JSH 2009) Hypertens Res. 2009;32(1):3-107.
- [Google Scholar]
- 2014 Evidence-based guideline for the management of high blood pressure in adults: report from the panel members appointed to the Eighth Joint National Committee (JNC 8) JAMA. 2014;311(5):507-520.
- [Google Scholar]
- Guidelines for the clinical use of 24 hour ambulatory blood pressure monitoring (ABPM) (JCS 2010): digest version. Circ J. 2012;76(2):508-519.
- [Google Scholar]
- Canadian Hypertension Society Guidelines for Ambulatory Blood Pressure Monitoring. Oxford University Press; 1999.
- [Google Scholar]
- Ambulatory blood pressure monitoring in Australia: 2011 consensus position statement. J Hypertens. 2012;30(2):253-266.
- [Google Scholar]
- Haemodynamic and radionuclide effects of amlodipine in coronary artery disease. Br J Clin Pharmacol. 1990;29(4):437-445.
- [Google Scholar]
- Intra-arterial monitoring of the antihypertensive effects of once-daily amlodipine. J Hum Hypertens. 1992;6(01):S9-S12.
- [Google Scholar]
- Management of hypertension with the fixed combination of perindopril and amlodipine in daily clinical practice: results from the STRONG prospective, observational, multicenter study. Am J Cardiovasc Drugs. 2009;9(3):135-142.
- [Google Scholar]
- Efficacy and safety of amlodipine/valsartan/hydrochlorothiazide single pill combination in Egyptian patients with hypertension uncontrolled on any dual therapy: an observational study. Curr Med Res Opin. 2020;36(4):537-544.
- [Google Scholar]
- A comparative study of the efficacy of cilnidipine and amlodipine used for the treatment of hypertension at tertiary health-care center. Natl J Physiol Pharm Pharmacol. 2019;9(5):454-458.
- [Google Scholar]
- Monotherapy with amlodipine or hydrochlorothiazide in patients with mild to moderate hypertension: comparison of their efficacy and effects on electrolytes. Malawi Med J. 2017;29(2):108-112.
- [Google Scholar]




