
Translate this page into:
Shared Airway for Tracheal Resection and Anastomosis in a Patient with Severe Subglottic Stenosis after Intra-cardiac Repair for Tetralogy of Fallot
*Corresponding author: Sambhunath Das, Department of Cardiac Anaesthesia and Critical Care, All India Institute of Medical Science, New Delhi, Delhi, India. sambhunathds833@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Anandan V, Das S. Shared Airway for Tracheal Resection and Anastomosis in a Patient with Severe Subglottic Stenosis after Intra-cardiac Repair for Tetralogy of Fallot. J Card Crit Care TSS. 2024;8:165-8. doi: 10.25259/JCCC_54_2023
Abstract
Subglottic stenosis is a condition causing narrowing of the trachea, which can occur rarely secondary to trauma, infection, tumors, inflammatory, and iatrogenic causes. In our case, the child developed subglottic stenosis post-cardiac surgery after being mechanically ventilated in the postoperative period. The causes for subglottic stenosis may be some trauma in the presence of coagulation abnormalities in cyanotic heart diseases such as TOF, the ischemia to the subglottic tissue by reduced perfusion during cardiopulmonary bypass, and/or the trauma caused by crying and fighting of the child while being with the endotracheal tube. Anesthetic management of the surgery is challenging for the anesthesiologist due to the shared airway by the surgeon and the anesthesiologist. The inability to effectively ventilate the patient after induction of general anesthesia will result in catastrophic complications. Subglottic stenosis requires careful planning and execution along with proper communication between the team.
Keywords
Subglottic stenosis
Shared airway
Airway management
Tracheal resection and anastomosis

INTRODUCTION
Subglottic stenosis is a condition causing the narrowing of the trachea. It occurs secondary to trauma, infection, tumors, inflammatory, or iatrogenic causes.[1] It will clinically present as symptoms of inspiratory airway obstruction including cough, shortness of breath, and stridor which worsens with activity. Prolonged mechanical ventilation in the postoperative period is also an uncommon cause of subglottic stenosis in the late postoperative period.[2] The condition will result in lifelong morbidity for the patient. Tracheal resection and anastomosis are the management of choice in these patients.
Anesthetic management of tracheal resection and anastomosis is a challenge for anesthesiologists. The tracheal lumen may be very small, even for the passage of the smallest endotracheal tube. The focus is on the airway, and maintaining ventilation during general anesthesia is difficult. Here, the airway is shared by the surgeon and the anesthesiologist. The inability to effectively ventilate the patient after induction of general anesthesia will result in catastrophic complications.[3] We describe the anesthetic management of tracheal resection and anastomosis in a child with subglottic stenosis after tracheal intubation for congenital cardiac surgery.
CASE REPORT
A 16-month-old boy, a known case of post-operative intracardiac repair (ICR) for Tetralogy of Fallot (TOF), was reported to be a casualty with a history of cough, rapid, and noisy breathing. There was no history of fever. On detailed history elaboration, it was found that oro-tracheal intubation was done on the day of ICR and was mechanically ventilated for 2 days. The patient was weaned off from ventilator and extubated. Post-extubation, the child had a lower respiratory tract infection treated with intravenous antibiotics and was observed in the intensive care unit and then in the ward for the next 17 days and was discharged.
The child again presented to the casualty with complaints of respiratory distress and noisy breathing after 5 days. On examination, the child had stridor and respiratory rate (RR) of 36/min, with subcostal and intercostal retractions. The child was admitted and a detailed evaluation was done. Chest X-ray PA view revealed the collapse of the right upper lobe [Figure 1] and an X-ray soft tissue of the neck showed upper tracheal stenosis [Figure 2]. He was further evaluated using flexible bronchoscopy which revealed severe membranous subglottic stenosis [Figure 3]. The child was scheduled for tracheal resection and anastomosis with general anesthesia.

- (a) Chest X-ray PA view showing right upper lobe collapse; (b) X-ray soft tissue of neck lateral view showing tracheal stenosis.
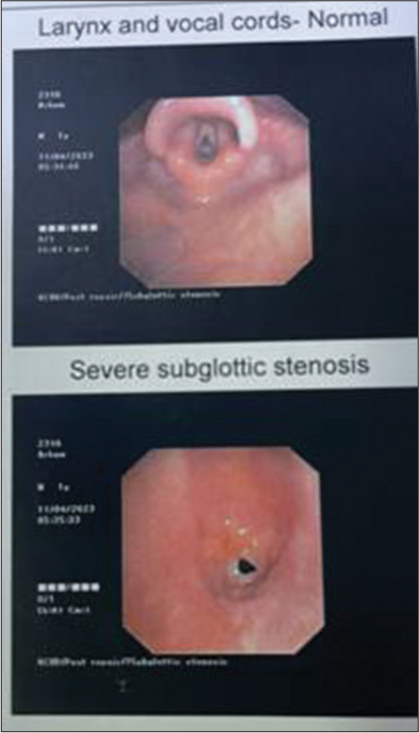
- Bronchoscopy views showing normal vocal cord (upper one) and severe membranous subglottic stenosis (lower one).
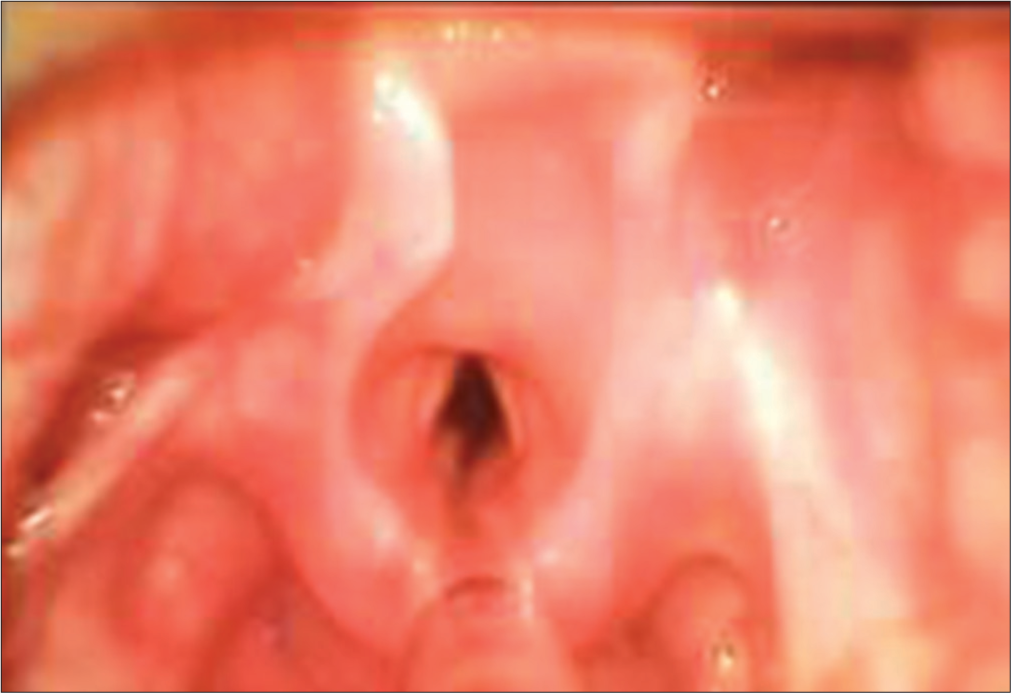
- Video laryngoscopy image of vocal cord with endotracheal tube in situ.
Anesthetic management
The child was premedicated with syrup midazolam 0.5 mg/kg; 30 min before being taken into the operation room. On the OR, standard ASA monitors were attached (electrocardiogram, oxygen saturation, and non-invasive blood pressure). A 24G intravenous line was secured in the left hand. Inj. Ketamine 2 mg/kg with glycopyrrolate 0.005 mg/kg was administered. Spontaneous ventilation was maintained with 100% oxygen. Anesthesia was provided using Sevoflurane (MAC 0.5–1). C-MAC video laryngoscope (8403 ZX) D blade – size 2 was used for intubation. On laryngoscopy, the vocal cords were seen as normal, and subglottic stenosis was also visualized approximately 1 cm below the vocal cord [Figure 3]. A 2.5 mm size endotracheal tube could be negotiated past the stenosis and the child was being successfully ventilated with a peak airway of 56 cmH2O. Inj. Rocuronium 0.9 mcg/kg and Inj. Fentanyl 2 mcg/kg were administered and the child was mechanically ventilated using FiO2 – 0.5, tidal volume – 6 ml/kg, and respiratory rate of 40/min.
After this, the Ear, Nose, and Throat (ENT) team proceeded with a tracheotomy, through which a bigger size endotracheal tube (size 4.0) could be passed and ventilation was maintained through this tube [Figure 4]. The ENT team went on with the tracheal resection of the stenosed portion. Once the posterior anastomosis was finished, again video laryngoscopy was done and a 4 mm ID uncuffed endotracheal tube was placed orally and anastomosis was completed over this tube. The patient was electively ventilated for 6 days postoperatively and was extubated on the 7th day, and the subsequent course was uneventful.

- Appropriate size endotracheal tube inserted through tracheotomy site.
DISCUSSION
Subglottic stenosis can occur secondary to insults such as trauma, inflammation, or infection. Symptoms can vary from cough with expectoration to severe dyspnea and stridor. It causes severe morbidity to the patient and in most cases will have to undergo tracheal resection and anastomosis. Tracheal resection and anastomosis, the surgery itself carries a lot of risk elements and can even end up in catastrophic complications.[4] An anesthesiologist has to maintain the patient’s airway and ventilation in the same anatomical space in which the surgeon operates. This is called shared airway anesthesia. One may have to depend on different strategies such as monitored anesthesia care, mask ventilation, supraglottic airway, insufflation with spontaneous breathing, and jet ventilation for the safe conduct of the case.[5,6]
In the present case, the child had developed subglottic stenosis in the postoperative period after cardiac surgery. The child was ventilated only for 2 days after surgery but still had to suffer the morbidity. The etiology behind the development of tracheal stenosis may be some trauma in the presence of coagulation abnormalities in cyanotic heart diseases such as TOF, the ischemia to the subglottic tissue by reduced perfusion during cardiopulmonary bypass, and/or the trauma caused by crying and fighting of the child while being with the endotracheal tube. The stenosis might have been of a lesser degree without clinical manifestation at first discharge from the hospital. Subsequently, the scar might have increased to a significant stage to cause stridor. The typical presentation of noisy breathing with tachypnea and tachycardia without fever pointed toward an airway obstruction, which could rightly be diagnosed using imaging modalities. Upper airway surgeries are always challenging for the anesthesiologist. In this case, spontaneous ventilation was maintained until we could secure an airway device for effective ventilation.
CONCLUSION
Tracheal stenosis requires careful planning and execution along with proper communication between the surgical and anesthesia team. This will help in providing safe anesthesia for the patient preventing catastrophic complications such as inadequate ventilation and hypoxemia. Strict adherence to these principles helped us in the safe conduct of anesthesia.
Acknowledgment
We thank Dr. Tanya Mital and Dr. Akshya for their presence during the management of the case.
Ethical approval
Institutional Review Board approval is not required.
Declaration Of Patient Consent
Patient consent is not required as patient identity is not disclosed or compromised.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
Financial support and sponsorship
Nil.
References
- Anesthesia Airway Management for Tracheal Resection and Reconstruction: A Single-center Case Series. Ann Palliat Med. 2021;10:3354-63.
- [CrossRef] [PubMed] [Google Scholar]
- Tracheal Stenosis after Prolonged Intubation Due to COVID-19. J Cardiothorac Vasc Anesth. 2022;36:2948-53.
- [CrossRef] [PubMed] [Google Scholar]
- Anaesthesia for Tracheal Resection and Anastomosis. J Anaesthesiol Clin Pharmacol. 2022;38:48-57.
- [CrossRef] [PubMed] [Google Scholar]
- Shared Airway: Techniques, Anesthesia Considerations, and Implications In: Fox C 3rd. Cornett E, Ghali G, editors. Catastrophic Perioperative Complications and Management. Cham: Springer; 2019.
- [CrossRef] [Google Scholar]
- Anesthesia for the Patient with Tracheal Stenosis. Anesthsiol Clin. 2010;28:157-74.
- [CrossRef] [PubMed] [Google Scholar]
- Resection and Reconstruction of the Trachea for the Treatment of Upper Tracheal Stenosis: Tracheal Versus Non-Tracheal Intubation. J Coll Physicians Surg Pak. 2018;28:879-81.
- [CrossRef] [PubMed] [Google Scholar]




