
Translate this page into:
Giant Subclavian Artery Aneurysm

*Corresponding author: Chinmaya Nanda, Department of Cardiac Anesthesia, Institute of Critical Care and Anesthesiology, Medanta the Medicity, Gurugram, Haryana, India. nandachinu@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Nanda C, Singh A, Mehta Y. Giant Subclavian Artery Aneurysm. J Card Crit Care TSS. 2024;8:48-50. doi: 10.25259/JCCC_60_2023
Abstract
Subclavian artery aneurysms are rare peripheral aneurysms. A giant subclavian artery aneurysm can lead to compression of the trachea or brachial plexus, erosion of the lung causing hemoptysis, hoarseness of voice, dysphagia, Horner’s syndrome, and upper extremity deep vein thrombosis. Compression of the trachea and inability to ventilate the patient can be a real challenge for the anesthesiologist and must be anticipated. Computed tomographic angiography is a useful imaging modality for its diagnosis and to rule out additional aneurysms in the body.
Keywords
Subclavian artery aneurysm
Tracheal compression
Computed tomography angiography

INTRODUCTION
Subclavian artery aneurysms (SAAs) are uncommon, and they constitute approximately 0.13%– 0.5% of all aneurysms.[1] The well-established etiological factors for SAA include infection (mycotic, syphilitic, and tuberculosis), atherosclerosis, trauma, and post-stenotic dilatation as a result of thoracic outlet syndrome. We present here an interesting case of a giant SAA causing compression of the trachea and right phrenic nerve, resulting in hemidiaphragmatic palsy.
CASE
A 51-year-old man presented with chief complaints of difficulty in breathing and pain in the right upper limb, right shoulder, and right side of the neck for one month. The patient also had a history of fracture of right forearm bones following a fall in 2006 and a family history of aortic aneurysm in his brother. Evaluation of the patient included a chest X-ray, transthoracic echocardiography, computed tomography (CT) of the chest, and CT angiogram of the entire aorta and great vessels.
Chest X-ray revealed a compression in the upper part of the trachea, an opacity in the right apical region, and an elevated right dome of the diaphragm [Figure 1a] which became normal after surgery [Figure 1b]. There was a mild external compression and deviation of the upper trachea to the left side on a CT scan of the chest. CT angiogram revealed fusiform aneurysmal dilatation of the right subclavian artery measuring 7.2 × 7.0 × 5.7 cm, originating from its proximal part [Figure 2]. A transthoracic echocardiogram showed a left ventricular ejection fraction of 45% with mild global left ventricular hypokinesia. The decision for surgical repair of the SAA was taken and the patient gave written informed consent for the same.
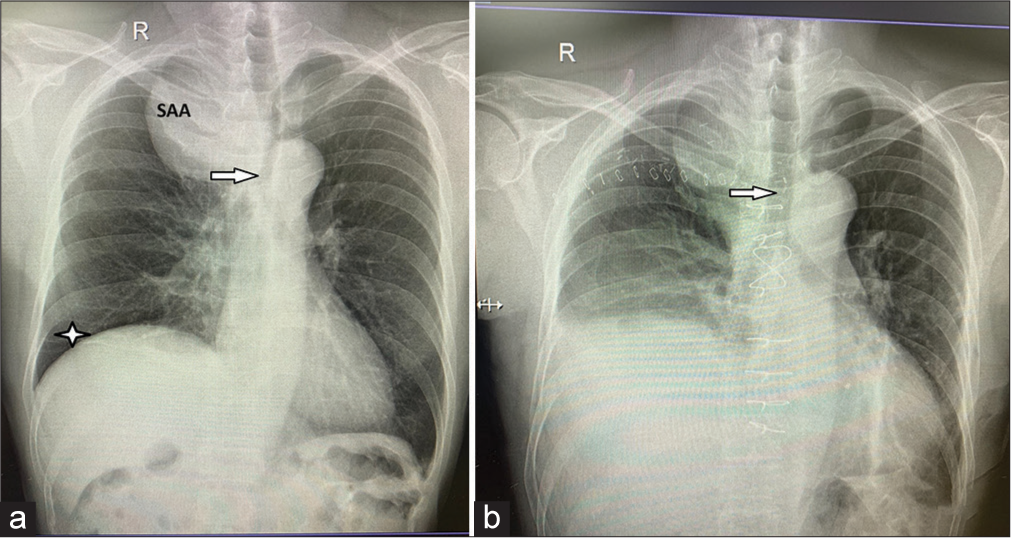
- Chest X-ray (a) depicting a large subclavian artery aneurysm, compression and leftward shift of the trachea (arrow), and elevated right hemidiaphragm (star). (b) Showing the normal course of the trachea after surgery (arrow).
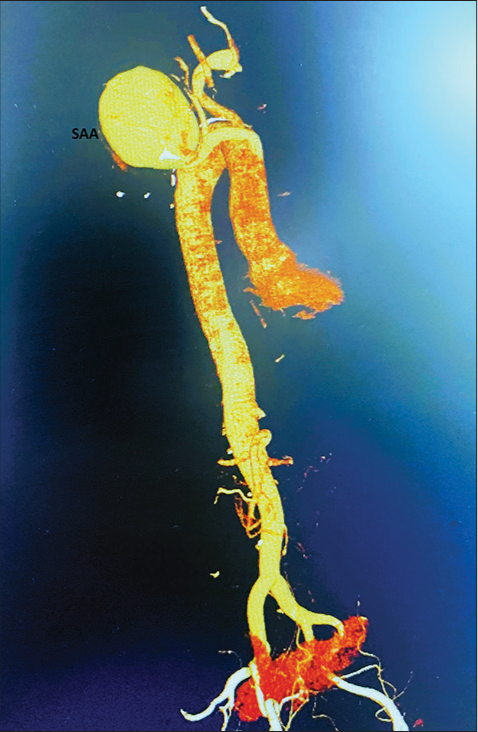
- Computed tomographic angiogram demonstrating a large subclavian artery aneurysm.
In the operation theater, after securing a wide-bore intravenous access, the right radial artery and left femoral artery were cannulated for arterial pressure monitoring. The right groin was dissected under local anesthetic infiltration. The right-sided femoral vessels were looped for the institution of emergency cardiopulmonary bypass (CPB) if required. Sevoflurane was used for the induction of anesthesia, and the tracheal intubation (8.0-mm endotracheal tube) was done in the spontaneously breathing patient. The patient could be ventilated without any difficulty. The chest was opened with a median sternotomy incision, and the subclavian artery was repaired with an 8-mm Intergard woven straight vascular graft (Maquet, Getinge Group, Goteborg, Sweden). The procedure was uneventful. The patient was extubated on the table, and the subsequent stay of the patient was unremarkable. The patient came to the outpatient department after one month for follow-up. He was asymptomatic, and the chest X-ray showed a normal trachea [Figure 1b].
DISCUSSION
Among all peripheral artery aneurysms, subclavian artery aneurysm is extremely uncommon. Giant SAAs (size >5 cm) are rare. It is seen more commonly in males and twice as common on the right than on the left side. Symptoms of a giant SAA may be related to compression of the trachea or brachial plexus, erosion of the lung causing hemoptysis, hoarseness of voice, dysphagia, Horner’s syndrome, and upper extremity deep vein thrombosis. In the presence of an arteriosclerotic peripheral aneurysm, multiple aneurysms are seen in 87% of the patients, emphasizing the usefulness of CT angiography to rule out additional aneurysms in the body.[1] Complete airway obstruction and cardiopulmonary arrest are catastrophic complications of mediastinal tumors and large aneurysms.[2] The airway obstruction can occur anytime in the perioperative period, e.g., during anesthetic induction, surgical procedure, tracheal extubation, or tilting of the patient during surgery. Airway maintenance is of utmost priority for the anesthesiologist in such a situation. In an emergency situation of irreversible airway obstruction, femoro-femoral CPB can be instituted before anesthetic induction to maintain oxygenation.[2]
Chest CT angiogram is not only helpful in the diagnosis of the aneurysm, site, and size, but it also helps in planning the surgical approach to repair the aneurysm.[3] It is essential to repair these aneurysms as spontaneous rupture and thrombosis is a risk if left untreated. Various surgical approaches have been described in the literature to address these aneurysms. They can be repaired by both open surgical and endovascular techniques.[4] Hybrid techniques and endovascular interventions, including the use of covered stents, have been reported in the literature.[4-6] The choice of approach should depend on the patient’s risk factors and the anatomy of the aneurysm.
CONCLUSION
In conclusion a giant SAA causing compression of the trachea can cause catastrophic airway obstruction in the perioperative period and must be anticipated.
Ethical approval
The Institutional Review Board approval is not required.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Conflicts of interest
Yatin Mehta is the member of the editorial board of the Journal.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
Financial support and sponsorship
Nil.
References
- Atherosclerotic Aneurysm of the Intrathoracic Subclavian Artery: A Case Report and Review of the Literature. J Vasc Surg. 1995;21:521-9.
- [CrossRef] [PubMed] [Google Scholar]
- Mediastinal Mass Resection: Femorofemoral Cardiopulmonary Bypass before Induction of Anesthesia in the Management of Airway Obstruction. J Cardiothorac Vasc Anesth. 2001;15:233-6.
- [CrossRef] [PubMed] [Google Scholar]
- Operation for Huge Subclavian Artery Aneurysm: A Case Report. J Thorac Dis. 2010;2:117-20.
- [Google Scholar]
- Peripheral Arterial Aneurysms: Open or Endovascular Surgery? Prog Cardiovasc Dis. 2013;56:36-56.
- [CrossRef] [PubMed] [Google Scholar]
- Hybrid Open and Endovascular Therapy for a Proximal Subclavian Artery Aneurysm. Vascular. 2008;16:236-8.
- [CrossRef] [PubMed] [Google Scholar]
- Endovascular Repair for Giant Right Subclavian Artery Aneurysm with Gore Viabahn and Pull-through Procedure: A Case Report. Front Surg. 2022;9:939818.
- [CrossRef] [PubMed] [Google Scholar]




