
Translate this page into:
Bovine Aortic Arch: Implications during Cardiac Surgery
*Corresponding author: Ajmer Singh, Department of Cardiac Anaesthesia, Medanta The Medicity, Gurugram, Haryana, India. ajmersingh@yahoo.com
-
Received: ,
Accepted: ,
How to cite this article: Singh A, Konalli VP, Nanda C. Bovine Aortic Arch: Implications during Cardiac Surgery. J Card Crit Care TSS. 2025;9:141-3. doi: 10.25259/JCCC_51_2024
Dear Editor,
The bovine aortic arch (BAA) is a vascular aberration in which the left common carotid artery (LCCA) arises either from the brachiocephalic trunk (BCT) or the LCCA and the BCT has a conjoined genesis from the aortic arch. It does not cause any symptoms in most cases because, typically, it is not associated with structural anomalies of the cardiovascular system. However, it may lead to a higher prevalence of ischemic, vascular, and neurologic problems in patients undergoing cardiovascular procedures. We recently encountered a BAA patient who underwent aortic valve replacement for severe aortic regurgitation. A 27-year-old man was found to have a common origin of BCT and LCCA on computed tomographic (CT) angiography of the aorta [Figures 1 and 2]. CT angiography was performed to exclude aortic dissection and aortic aneurysm as there was enlargement of the aortic root and ascending aorta (4.0 cm × 3.9 cm) on echocardiography. The surgical procedure was uneventful.
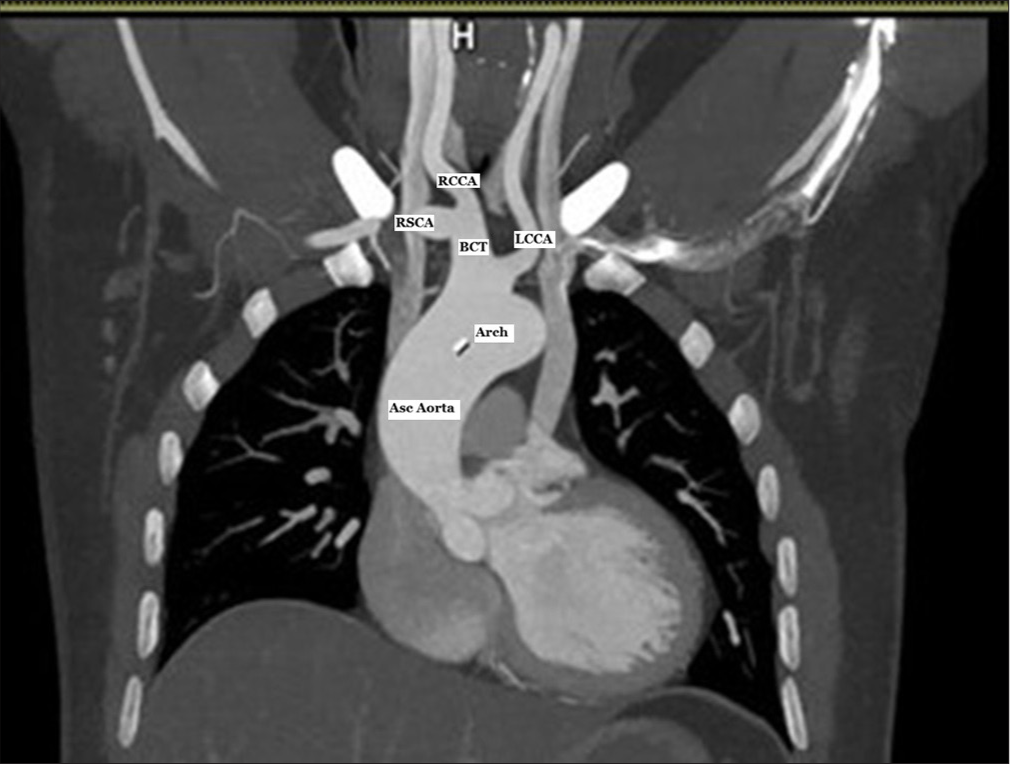
- Computed tomographic angiography of the aorta demonstrating the common origin of the BCT and the LCCA. Asc Aorta: Ascending aorta, RCCA: Right common carotid artery, RSCA: Right subclavian artery, BCT: Brachiocephalic trunk, LCCA: Left common carotid artery.
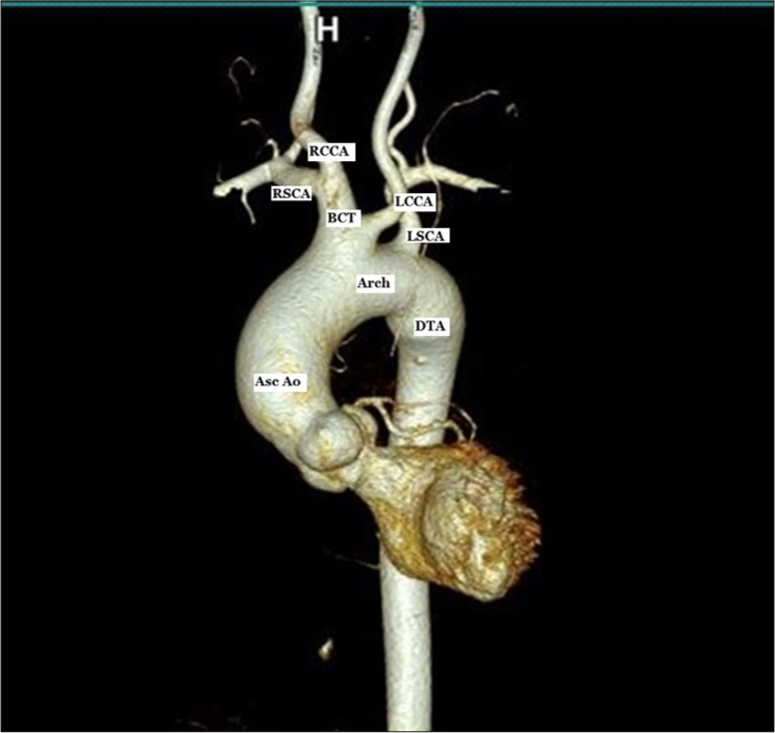
- Volume-rendered image of the computed tomographic angiography of the aorta showing the common origin of the BCT and the LCCA and separate origin of the LSCA. Asc Ao: Ascending aorta, DTA: Descending thoracic aorta, RSCA: Right subclavian artery, RCCA: Right common carotid artery, BCT: Brachiocephalic trunk, LCCA: Left common carotid artery, LSCA: Left subclavian artery.
The BAA is the second most common aberration of the branching pattern of the aortic arch in humans. Its two subtypes include (i) the conjoined genesis of BCT and LCCA from the arch of the aorta and (ii) LCCA originating from the BCT at a distance of 1–2.5 cm from the arch. The former subtype is more common than the latter. The BAA is seen in 1–35% of the general population, but the African and South American continents have the highest occurrence.[1] The patients with BAA have significantly higher rates of hypertension (91.8% vs. 76.1%) and thinner layers of tunica media. Consequently, they are at higher risks of aortic dilation/dissection, intramural hematoma, and stroke (24.5% vs. 10.2%) compared to patients with normal arch.[2] Furthermore, the BAA can independently identify the location of the entry site of the dissection tear in the aortic arch. This occurs presumably due to changes in the blood flow velocity and hemodynamics that may weaken the tissues of the arch of the aorta. In a study of 32 patients of type-A aortic dissection with BAA by Maxwell et al., a different perioperative approach was required for the institution of selective antegrade cerebral perfusion.[3] The surgical technique may need modification in terms of applying a clamp above or below the origin of the LCCA to produce unilateral or bilateral antegrade cerebral perfusion, respectively. The patients of type-B aortic dissection with BAA undergoing thoracic endovascular aortic repair are at a potential risk of retrograde aortic dissection.[4] The presence of BAA may also influence the choice of carotid artery stents, carotid artery revascularization, and endovascular graft required for arch vessel reconstruction. During cardiac catheterization of patients with BAA, familiarity with handling of hockey-stick catheters or recurved catheters such as Vitek, Simmons 1, or Simmons 2 is essential. Stenting of carotid arteries may be riskier in BAA patients due to the tight turn required to negotiate BCA and LCCA if femoral access is used. Therefore, patients with BAA may benefit from a brachial or a radial approach. Moreover, the neurologic complications, including minor/major stroke or transient ischemic attacks, after carotid artery stenting were more frequently seen in the BAA group (10.3% vs. 4.1%) versus normal arch group.[5, 6] The possible mechanisms for a higher incidence of stroke in BAA patients could be a much larger area of a single common conduit for passage of debris or flow alterations causing local thrombus formation. For patients undergoing interventional procedures such as transcatheter aortic valve implantation or carotid artery stenting, the use of distal or proximal cerebral embolic protection devices such as SENTINEL protection system or a two-filter deployment can be helpful. In an analysis of a large cohort of patients undergoing thoracic surgery, hemorrhage and ischemia were more commonly seen in patients with BAA by Popieluszko et al.[5]
In conclusion, identifying the BAA aberration is vital in patients undergoing cardiac surgery, as well as surgery or endovascular procedures of the aorta. Anatomical variations in the aortic arch are associated with increased rates of thoracic aortic diseases, aortic dissection, coarctation of aorta, and stroke, necessitating early diagnosis and increased supervision of patients with such incidentally observed anomalies.
Ethical approval
Institutional Review Board approval is not required.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
Financial support and sponsorship: Nil.
References
- Anatomical Variations in the Branches of the Human Aortic Arch in 633 Angiographies: Clinical Significance and Literature Review. Surg Radiol Anat. 2009;31:319-23.
- [CrossRef] [PubMed] [Google Scholar]
- In DeBakey Type I Aortic Dissection, Bovine Aortic Arch is Associated with Arch Tears and Stroke. Ann Thorac Surg. 2017;104:2001-8.
- [CrossRef] [PubMed] [Google Scholar]
- Congenital Anomalies of the Aortic Arch in Acute Type-A Aortic Dissection: Implications for Monitoring, Perfusion Strategy, and Surgical Repair. J Cardiothorac Vasc Anesth. 2014;28:467-72.
- [CrossRef] [PubMed] [Google Scholar]
- Retrograde Ascending Aortic Dissection as an Early Complication of Thoracic Endovascular Aortic Repair. J Vasc Surg. 2012;55:1255-62.
- [CrossRef] [PubMed] [Google Scholar]
- A Systematic Review and Meta-analysis of Variations in Branching Patterns of the Adult Aortic Arch. J Vasc Surg. 2018;68:298-306.
- [CrossRef] [PubMed] [Google Scholar]
- The Importance of TEE Examination in Patients with Pseudoaneurysm of Arch of Aorta Post-TEVAR Procedure. J Card Crit Care TSS. 2022;6:306.
- [CrossRef] [Google Scholar]




