
Translate this page into:
Ascariasis and Cardiac Surgery: A Case Report
Ajmer Singh, MD Institute of Critical Care and Anesthesiology, Medanta-The Medicity Sector-38, Gurugram, Haryana, 122001 India ajmersingh@yahoo.com
This article was originally published by Thieme Medical and Scientific Publishers Pvt. Ltd. and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Ascariasis is a common helminthic infection, particularly in the tropical countries. We describe a case of eosinophilia who underwent coronary artery bypass graft (CABG) surgery. Postoperatively, he was found to have ascaris lumbricoides in the oral cavity. Timely detection and removal of the worm prevented the possible complications such as airway obstruction, bronchospasm, lung collapse, or intestinal obstruction. The case emphasizes the importance of considering parasitic infection as a differential diagnosis in patients presenting with eosinophilia for elective surgery.
Keywords
Ascaris
Cardiac Surgery
Eosinophilia

Introduction
In the tropical countries, ascariasis is the most commonly seen helminthic infection, with an estimated prevalence of approximately 25%.1 Children and malnourished individuals with poor sanitation and personal hygiene are more commonly affected. Depending on its developmental stage, it can cause various complications such as airway obstruction, bronchospasm, pneumonitis, lung collapse, or intestinal obstruction in the perioperative period.1 Adult worms can migrate to some other sites, causing pancreatitis, biliary obstruction, cholangiohepatitis, liver abscess, appendicitis, intestinal perforation, granulomatous peritonitis, and ascaris empyema.2
Case Report
We describe a 43-year-old patient admitted for coronary artery bypass graft (CABG) surgery, who was found to have eosinophilia (differential eosinophils 13.6%, absolute eosinophil count 980 cells/mm3) on preoperative workup. Single dose of albendazole 400 mg was administered and the patient underwent off-pump CABG surgery. In the postoperative period, while on mechanical ventilation, the nurse noticed a large worm (~25 cm long) lying in the oral cavity, which was removed by forceps (Fig. 1). Close examination of the worm by microbiologist confirmed the diagnosis of ascaris lumbricoides (Fig. 2). The patient received anthelmintic therapy in the form of albendazole and ivermectin. Subsequent course in the hospital was uneventful.
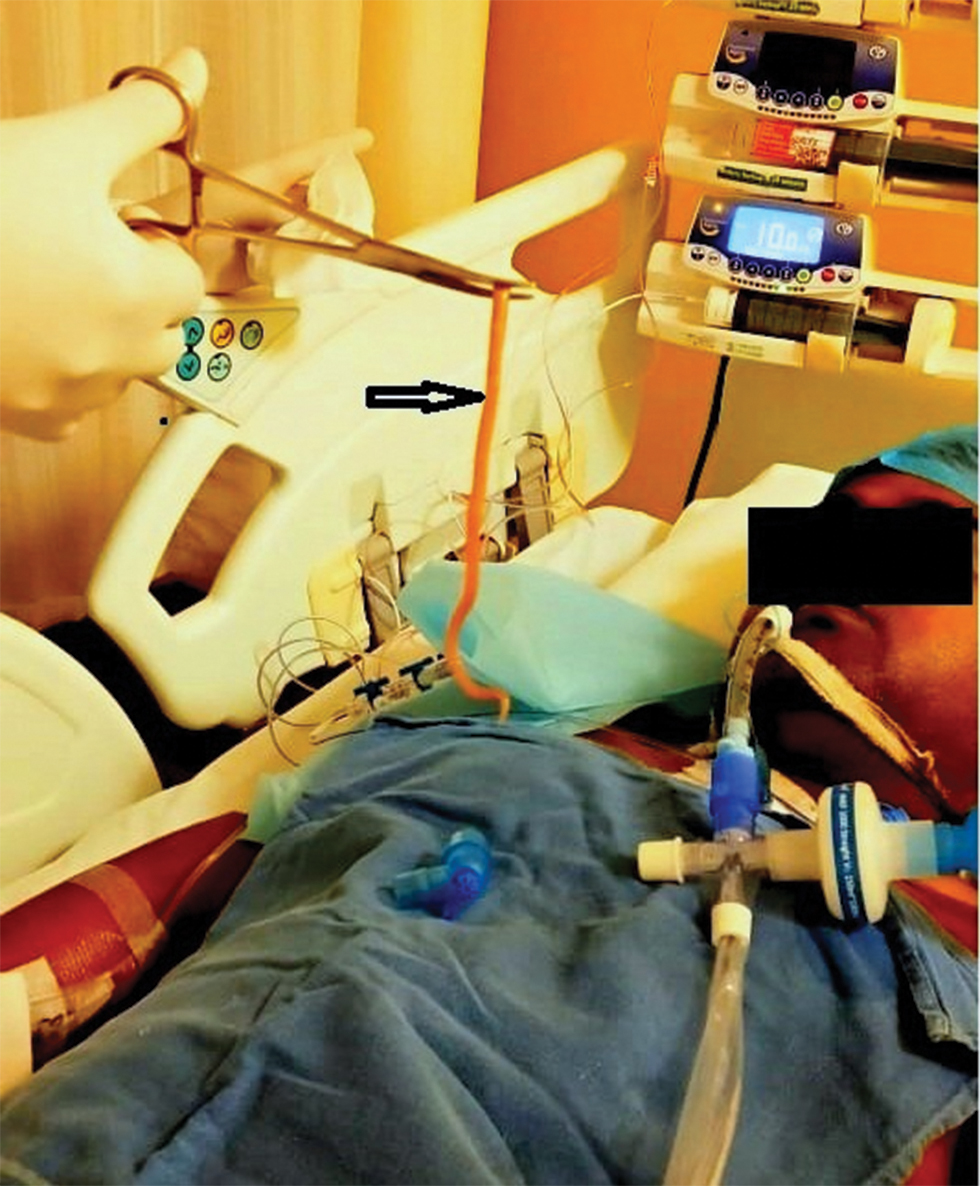
- An ascaris worm (arrow) removed from the oral cavity.
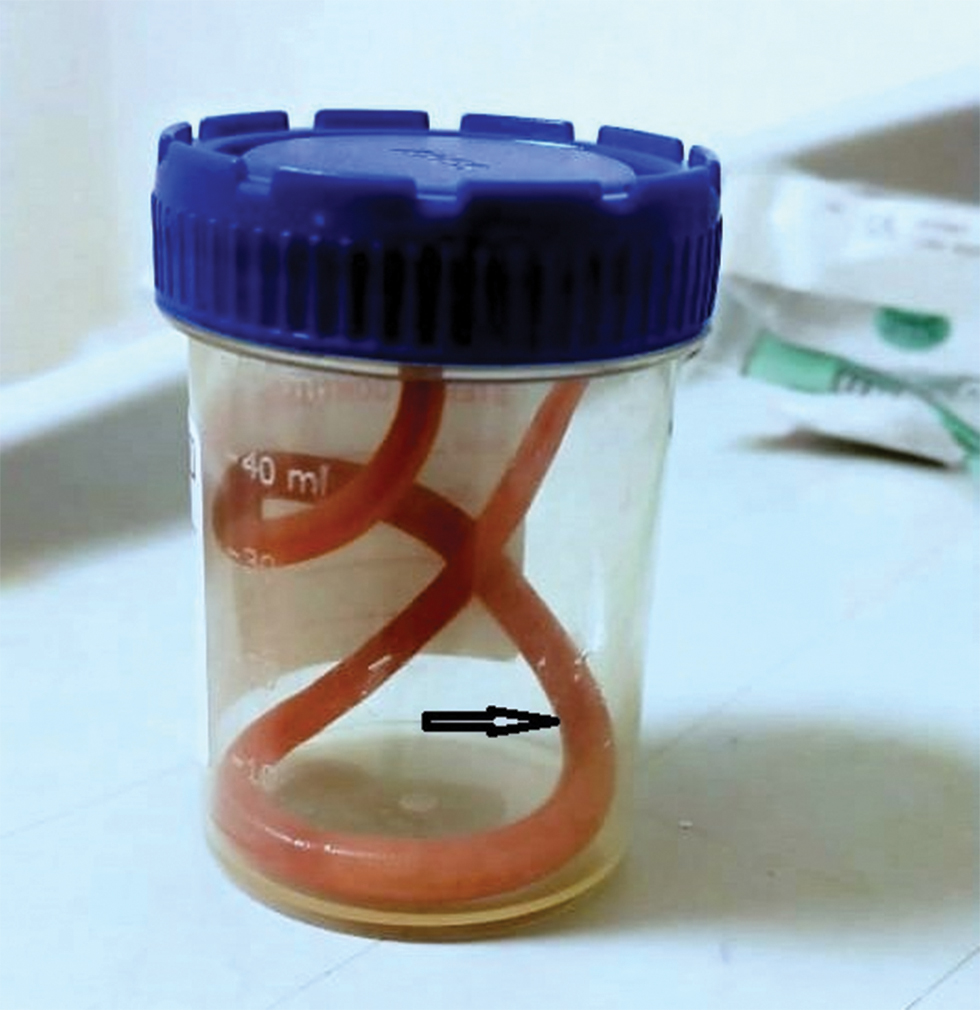
- Long Ascaris Lumbricoides worm (arrow).
Discussion
Most cases of ascaris lumbricoides are asymptomatic. Humans are affected by ingestion of eggs from contaminated food, water, and infected soil. The adult worms live in the jejunal lumen and are known to migrate into the most unusual locations in the body. The clinical spectrum of the disease involves pulmonary, intestinal, pancreatic, and hepatobiliary systems.3 Peripheral eosinophilia, resulting from larval invasion of the blood, is commonly seen. Therefore, presence of eosinophilia should raise the suspicion of ascaris infestation. The diagnosis is confirmed by stool examination, and the treatment consists of deworming with oral anthelmintics.
While peristalsis helps in passage of worms via stool, reverse peristalsis can push them into the oral cavity. Other possible mechanisms of upward migration after surgery include supine posture of the patient, relaxed esophageal sphincter, presence of nasogastric tube, absent swallowing reflex, cough reflex produced by deep suctioning of oropharynx, reduced gastric pH and pepsin release by the use of proton-pump inhibitors. Migration of adult worms up to the esophagus and subsequent entry into airway can also result from subtherapeutic anthelmintic therapy, irritation caused by anthelmintic drugs, and effect of anesthetic drugs.4 Ascaris seems to be particularly sensitive to anesthetic agents, as they stimulate the worm to be hypermobile.5 Fatal and near-fatal airway obstruction, obstruction of vocal cords, laryngospasm, and lung collapse have all been reported in extubated patients after aspiration of ascaris worm during coughing or vomiting.6, 7 Patients with altered sensorium, or those under effect of anesthesia/sedation, are more likely to suffer from fatal respiratory obstruction. Life-threatening airway obstruction has been reported even in intubated patients by migration of the worm into the trachea with noncuffed or loosely-fitted endotracheal tube.8 Serious, unexplained hyperthermia resulting from ascaris infection has been reported in a postoperative cardiac surgical patient.9
The case emphasizes the importance of adequate deworming before elective surgery in a patient of eosinophilia, particularly for those living in endemic areas. We also suggest to keep the head end of the patient elevated by 30 to 40°while on ventilator, in order to reduce the incidence of upward migration of the worm.
Conflicts of Interest
None declared.
References
- 1990. p. :2137-2138. Intestinal nematodes. In: Mandell GI, Douglas RG, Bennet JE, eds. Principles and Practice of Infectious Diseases. Edinburg: Churchill Livingstone
- Wandering ascaris coming out through the abdominal wall. Int J Prev Med. 2013;4(6):720-722.
- [Google Scholar]
- 2007. p. :1517-1520. Infectious diseases. Protozoal and helminthic infections. In: McPhee SJ, Papadakis MA, Turney LM Jr, eds. Current Medical Diagnosis Treatment. 46th ed. McGraw Hill (Medical)
- Anaesthesia and Ascaris pneumonia (Loeffler’s syndrome) Indian J Anaesth. 2015;59(2):125-126.
- [Google Scholar]
- Near fatal respiratory obstruction due to Ascaris lumbricoides. Trop Doct. 2005;35(3):185.
- [Google Scholar]
- Ascaris lumbricoides infection causing respiratory distress after coronary artery bypass grafting. Surg Infect (Larchmt). 2010;11(2):177-178.
- [Google Scholar]
- Airway obstruction by round worm in mechanically ventilated patient: An unusual cause. Indian J Anaesth. 2011;55(6):637-638.
- [Google Scholar]
- Hyperthemia after cardiac surgery due to ascariasis in a child: report of a case. Gen Thorac Cardiovasc Surg. 2012;60(7):446-448.
- [Google Scholar]




