
Translate this page into:
Comparison of Yoga Versus Sports Activities in Improving Cardiac Autonomic Function in Adolescents with Perceived Anxiety: A Comparative Randomized Pilot Study
 , Sai lakshmi D2, Archana Devi K S2, Swetha V2, Glady Cormel A2, Sasidharan T2, Divya Dharshini T2, Mohana Priya S2, Girish P2
, Sai lakshmi D2, Archana Devi K S2, Swetha V2, Glady Cormel A2, Sasidharan T2, Divya Dharshini T2, Mohana Priya S2, Girish P2
*Corresponding author: E. Thirumurugan, Assistant Professor, Department of Cardiology, Dr. M.G.R Educational and Research Institute, Chennai, Tamil Nadu, India. thiruahs1002@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Thirumurugan E, lakshmi SD, Devi KSA, Swetha V, Cormel AG, Sasidharan T, et al. Comparison of Yoga Versus Sports Activities in Improving Cardiac Autonomic Function in Adolescents with Perceived Anxiety: A Comparative Randomized Pilot Study. J Card Crit Care TSS. 2025;9:99-109. doi: 10.25259/JCCC_1_2025
Abstract
Objectives
Heart rate variability (HRV) is a non-invasive metric to assess the psycho-physiological fluctuations in the temporal intervals between successive heartbeats. This measure offers valuable insights into the dynamic equilibrium between the activities of the sympathetic and parasympathetic nervous systems. In the academic setting, stress can negatively impact psychological well-being, potentially resulting in emotional distress and reduced cognitive function and learning abilities. Failure to seek treatment for an extended period may result in irreversible changes in autonomic functions, leading to significant alterations in cardiovascular health. The primary aim of this research was to evaluate the effects of yoga and sports activities on cardiac autonomic function in adolescents who are experiencing anxiety.
Materials and Methods
The interventional study occurred at the Department of Allied Health Science in a private medical college and hospital in Chennai, Tamil Nadu. The study included forty adolescent students (aged 19–24) with reported anxiety that attended a paramedical college and had no previous exposure to yoga and sports activities.
Results
Significant differences were identified across several parameters within the yoga group following eight sessions, notably in standard deviation of the normal-to-normal intervals (SDNN), mean RR interval, mean heart rate, root mean square of successive differences between successive normal heartbeats, MxDMN, and pNN50. The yoga group demonstrated a statistically significant reduction in SDNN parameters compared to baseline measurements after the eighth session, which strongly suggests an enhanced capacity for stress management attributable to the yoga interventions. In contrast, the sports group did not exhibit any significant changes in SDNN, mean RR interval, or MxDMN, as P-values remained above the threshold of 0.05.
Conclusion
The research identified a notable enhancement in cardiac autonomic function, signifying that Yoga positively influences an individual’s overall health.
Keywords
Autonomic nervous system
Heart rate variability
Sports
Stress
Yoga

INTRODUCTION
The educational environment in India is renowned for fostering a culture of academic excellence, motivating Indian students to pursue high achievement. This pursuit often results in heightened levels of stress.[1,2] Medical college students, in particular, face demanding academic requirements that increase stress levels, impacting their overall health and well-being.[3] Unlike typical adolescent worries, stress poses a more substantial concern for medical students.[4] According to the Job Demand-Control-Support model, stress escalates in high demand, low self-control, and low social support.[5] In the academic domain, stress can detrimentally affect psychological health, potentially leading to mental distress and impaired cognitive function and learning.[6] The absence of treatment for an extended period can lead to irreversible changes in autonomic functions, which can cause significant alterations in cardiovascular functions.
Cardiovascular diseases significantly burden public health in both developed and developing nations.[7] Various cardiovascular ailments, including hypertension, arrhythmias, and metabolic dysfunction, often originate from an autonomic nervous system (ANS) imbalance.[8,9] Heart rate variability (HRV) is a non-invasive method for assessing cardiac autonomic activity. This parameter reflects the equilibrium between sympathetic and parasympathetic control of the heart, measured through normal-to-normal (NN) intervals. Reduced parasympathetic activity contributes to diminished HRV, a critical clinical indicator for hypertension and coronary artery disease.[10,11]
Yoga contributes to establishing equilibrium in ANS activity, as indicated by sympathovagal balance, thereby demonstrating an enhancement in HRV. Yoga elicits the relaxation response, physiologically antithetical to the stress or fight-or-flight response. Consequently, this elicits a decline in sympathetic nervous system activity while enhancing parasympathetic activity.[12] In contrast, activities such as Dodgeball engage the sympathetic nervous system, triggering the body’s fight or flight response. Despite this, such activation can still reduce stress through several mechanisms. Physical activities, including Dodgeball participation, lead to endorphins release, acting as natural mood enhancers. These substances are crucial in combating stress and enhancing overall mood.[13] The primary aim of this research was to evaluate the effects of yoga and sports activities on cardiac autonomic function in adolescents who are experiencing anxiety.
MATERIAL AND METHODS
The prospective interventional study was conducted at the Department of Allied Health Science (AHS) within a private medical college and hospital in Chennai, Tamil Nadu, following full approval from the Institutional Scientific and Ethics Committee for the clinical protocol. This study engaged forty adolescent students, aged 19–24, from a paramedical college, all of whom were identified as experiencing perceived anxiety and had no prior yoga experience. Utilizing the depression, anxiety, and stress scale (DASS-42) questionnaire alongside the Welltory app (version 3.2.3), we successfully identified students with perceived anxiety, selecting those who displayed moderate to severe levels for participation. Participants who regularly engage in athletic activities, smoke, have a history of alcohol dependency, are experiencing acute illnesses, or have recently undergone surgical procedures were definitively excluded from the study. Furthermore, individuals diagnosed with endocrine disorders, cardiovascular conditions, chronic obstructive pulmonary disease, or asthma, as well as those who engage in more than 1 h of regular physical exercise, were also excluded from maintaining a strictly controlled study environment. After thorough baseline testing confirmed a normal body mass index (BMI), students were randomly assigned to either the yoga or sports group, with 20 participants in each. Before the experiment, all participants provided comprehensive written informed consent and received detailed instructions on the study procedures. Data collection occurred in the AHS Skill laboratory, where participants utilized cutting-edge Photoplethysmography (PPG) technology. The Welltory app, a specialized smartphone application designed to measure HRV through PPG technology, was integral to our data-gathering process. PPG technology uses a light-emitting diode, commonly a smartphone camera flash, to assess heart rate (HR) by analyzing skin illumination and collecting HRV time domain data (standard deviation of the normal-to-normal intervals [SDNN], root mean square of successive differences between successive normal heartbeats [RMSSD]).[14] Participants in the study received detailed and explicit instructions from experts regarding the maintenance of their regular sleep routines and guidance to refrain from consuming caffeine and alcohol before the assessments. The evaluations were systematically scheduled for the morning hours, followed by a light breakfast, stipulating that participants consume this meal at least 2 h before the assessments. Participants were instructed to empty their bladders before the start of the recordings. Each participant completed the DASS-42 questionnaire confidently before and after the 4-week intervention.[15] During HRV measurements, participants maintained a supine position with their eyes open to ensure the highest accuracy in the data collected. This standardized protocol was consistently applied for baseline measurements throughout the 4-week study, encompassing 2 weekly sessions.
Randomization and blinding/masking
Three hundred and twenty potential subjects were screened to assess eligibility for the study; however, 270 individuals did not fulfill the established criteria. As a result, 50 participants remained, randomly assigned to one of two groups: the yoga group, consisting of 25 participants, and the sports group, comprising 25 participants. During the follow-up phase, five participants from each group were withdrawn from the study due to health-related issues and non-compliance with the prescribed training sessions [Figure 1]. The allocation process was implemented using a simple randomization technique comparable to a coin toss, ensuring an unbiased selection methodology. In the current study, participants were informed of their group assignments, while the investigator remained unaware of the identities of the group members, thereby achieving a double-blind design. Certified and qualified yoga instructors facilitated the sessions, while experienced physical education trainers supervised the sports sessions. A skilled medical physiologist evaluated the parameters of HRV to mitigate potential observer discrepancies.
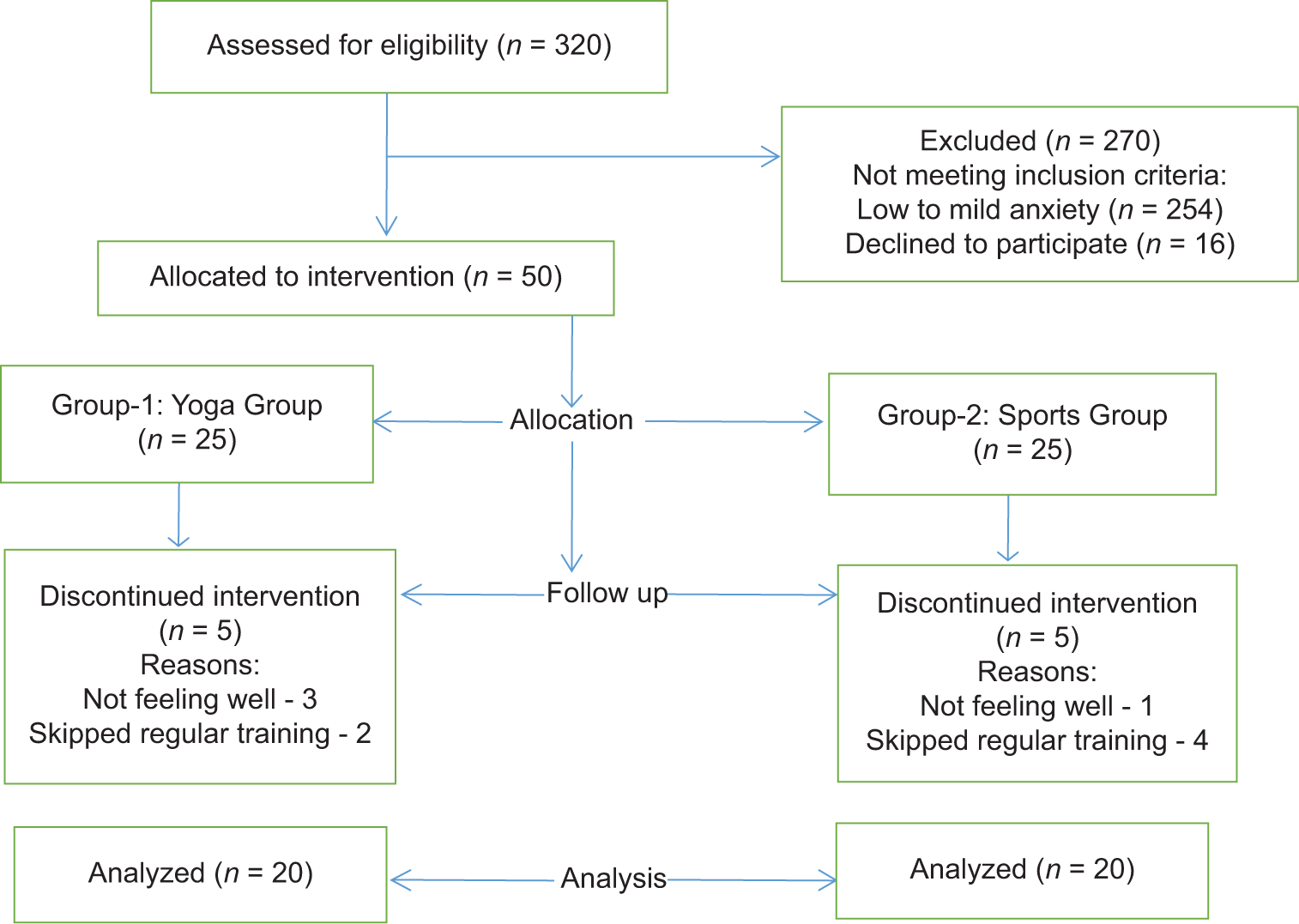
- Flow chart diagram.
Intervention
The entire yoga session lasted for an hour and involved all 20 students in the yoga group practicing various forms of hatha yoga. Each session began with Surya Namaskar (sun salutation) followed by balasana (child pose), uttanasana (standing yoga pose), ustrasana (camel pose), virabhadrasana (warrior pose), chakrasana (wheel pose), ardha pincha mayurasana (dolphin pose), halasana (plough pose), vrikshasana (tree pose), and padmasana (lotus pose) for 40 min. The students then participated in a 15-min meditation session, concluding with a 5-min shavasana (relaxation exercise) while lying on the floor. The students participated in a Dodgeball (Sports) activity where two teams aimed to hit their opponents with the ball. Before the session began, the students engaged in a 10-min warm-up exercise. Each team played continuously for 10 min inside and 10 min outside the ring, for a total session duration of 40 min. After the activity, the students underwent a 10-min relaxation exercise to unwind and rest.
Outcome measures
In this study, our main focus was on HRV as the primary outcome measure. We analyzed linear model HRV, examining time domains. Time domain analysis encompasses the evaluation of several critical metrics, including the SDNN, the square root of the mean squared differences between consecutive NN intervals (RMSSD), the count of interval differences exceeding 50 ms (NN50), and the ratio calculated by dividing NN50 by the total number of NN intervals, known as pNN50.
Statistical analysis
The statistical analysis was executed utilizing IBM SPSS Statistics version 20. The descriptive variables will encompass all explanatory and outcome variables, employing means and standard deviations (SD) for quantitative variables, as well as frequencies (N) and percentages (%) for categorical variables. The independent t-test will evaluate differences between groups concerning continuous variables. Furthermore, the paired-sample t-test will analyze differences between pre-intervention and post-intervention outcomes. The Chi-square test was utilized as necessary within the context of the analysis. A significance level of P < 0.05 will be established to determine statistical significance in the presented analysis framework.
Post hoc analysis
We utilized G*Power version 3.1.9.4 to estimate the sample size required for our study, focusing on the HRV parameter, specifically the Mean Overall Dynamic Activity (MODA), after the intervention. The results indicated that the MODA for participants engaged in yoga was 727.5 (±108.1), while for those involved in sports, it was 548.3 (±174.8). We calculated an effect size (d) of 1.2330699 based on the mean values and SDs. The significance level (α) was set at 0.05, with a desired power (1 - β) of 0.95 and an allocation ratio (N2/N1) of 1. Consequently, we estimated a sample size of 19 participants in each group, totaling 38 participants, while achieving an actual power of 0.95.
RESULTS
The study recruited 40 participants who met the established inclusion and exclusion criteria. The participants had a mean age of 19.4 years, with a SD of ± 0.6 years, and were randomly allocated into two distinct groups: one group engaged in yoga (n = 20) and the other participated in sports (n = 20). The mean age (SD) was 19.4 ± 0.6 years in the yoga group and 19.5 ± 0.6 years in the sports group. No significant differences were found between the yoga and sports groups regarding age, height, weight, BMI, and oxygen saturation (SpO2), suggesting a similar distribution of subjects in both groups (P > 0.05) [Table 1].
| Variables | Group | Mean±SD | T-statistic (t) | Degree of freedom (df) | Mean difference | 95% confidence interval of the difference | P-value | |
|---|---|---|---|---|---|---|---|---|
| Lower | Upper | |||||||
| Age | Yoga | 19.45±0.60 | −0.261 | 38 | −0.05 | −0.438 | 0.338 | 0.79 |
| Sports | 19.50±0.60 | 38 | ||||||
| Height | Yoga | 159.30±8.00 | −0.075 | 38 | −0.20 | −5.615 | 5.21 | 0.94 |
| Sports | 159.50±8.89 | 37.5 | ||||||
| Weight | Yoga | 61.43±13.49 | 1.324 | 38 | 5.82 | −3.081 | 14.72 | 0.19 |
| Sports | 55.61±14.30 | 37.8 | ||||||
| BMI | Yoga | 24.24±5.44 | 0.978 | 38 | 1.62 | −1.73 | 4.98 | 0.33 |
| Sports | 22.62±5.06 | 37.8 | ||||||
| SpO2 | Yoga | 97.55±2.35 | −1.644 | 38 | −0.90 | −2.008 | 0.208 | 0.10 |
| Sports | 98.45±0.68 | 22.2 | ||||||
SD: Standard deviation, BMI: Body mass index
Result of time domain of HRV in yoga group
The initial SDNN (ms) value for the yoga group was 266.1 ± 85.9 (ms). Subsequent SDNN values at the 4th and 8th sessions were recorded as 147.60 ± 109.06 and 136.10 ± 111.83 (ms), respectively. A statistically significant reduction in SDNN (ms) values was observed in the yoga group following the eighth session compared to baseline data [Table 2 and Figure 2].
| Variables | Mean±SD | 95% confidence interval of the difference | T-statistic | Degree of freedom (df) | P-value | |
|---|---|---|---|---|---|---|
| Lower | Upper | |||||
| SDNN | ||||||
| Pre versus S4 | 266.10±85.99 | 51.689 | 185.311 | 3.71 | 19 | 0.00* |
| 147.60±109.06 | ||||||
| S4 versus S8 | 147.60±109.06 | −57.141 | 80.141 | 0.35 | 19 | 0.73 |
| 136.10±111.83 | ||||||
| Pre versus S8 | 226.10±85.99 | 79.79 | 180.206 | 5.42 | 19 | 0.00* |
| 136.10±111.83 | ||||||
| Mean RR | ||||||
| Pre versus S4 | 913.30±150.69 | 12.99 | 224.80 | 2.350 | 19 | 0.03* |
| 794.40±161.78 | ||||||
| S4 versus S8 | 794.40±161.78 | −74.85 | 100.05 | 0.302 | 19 | 0.76 |
| 781.80±139.29 | ||||||
| Pre versus S8 | 913.30±150.69 | 57.19 | 205.81 | 3.704 | 19 | 0.00* |
| 781.80±139.29 | ||||||
| RMSSD | ||||||
| Pre versus S4 | 216.75±131.135 | −16.47 | 168.67 | 1.721 | 19 | 0.10 |
| 140.65±106.35 | ||||||
| S4 versus S8 | 140.65±106.35 | −78.52 | 100.82 | 0.260 | 19 | 0.79 |
| 129.50±141.85 | ||||||
| Pre versus S8 | 216.75±131.135 | 20.43 | 154.06 | 2.733 | 19 | 0.01* |
| 129.50±141.85 | ||||||
| PNN50 | ||||||
| Pre versus S4 | 68.85±24.515 | −4.87 | 28.87 | 1.488 | 19 | 0.15 |
| 56.85±32.218 | ||||||
| S4 versus S8 | 56.85±32.218 | −11.56 | 29.06 | 0.902 | 19 | 0.37 |
| 48.10±32.148 | ||||||
| Pre versus S8 | 68.85±24.515 | 5.50 | 35.99 | 2.849 | 19 | 0.01* |
| 48.10±32.148 | ||||||
| MXDMN | ||||||
| Pre versus S4 | 0.85±0.366 | 0.259 | 0.7400 | 4.359 | 19 | 0.00* |
| 0.35±0.48 | ||||||
| S4 versus S8 | 0.35±0.48 | −0.288 | 0.188 | −0.438 | 19 | 0.66 |
| 0.400±0.50 | ||||||
| Pre versus S8 | 0.85±0.366 | 0.211 | 0.688 | 3.943 | 19 | 0.00* |
| 0.400±0.50 | ||||||
| MODA | ||||||
| Pre versus S4 | 714.75±185.09 | −146.64 | 71.14 | −0.726 | 19 | 0.47 |
| 752.50±152.58 | ||||||
| S4 versus S8 | 752.50±152.58 | −47.62 | 97.62 | 0.721 | 19 | 0.48 |
| 727.50±108.18 | ||||||
| Pre versus S8 | 714.75±185.09 | −112.25 | 86.75 | −0.268 | 19 | 0.79 |
| 727.50±108.105 | ||||||
| Heart rate | ||||||
| Pre versus S4 | 69.55±13.43 | −18.74 | 0.748 | −1.93 | 19 | 0.06 |
| 78.55±16.44 | ||||||
| S4 versus S8 | 78.55±16.44 | −9.63 | 8.532 | −0.127 | 19 | 0.90 |
| 79.10±13.52 | ||||||
| Pre versus S8 | 69.55±13.43 | −15.95 | −3.14 | −3.122 | 19 | 0.00* |
| 79.10±13.52 | ||||||
Bold and * indicates: Statistically significant at P<0.05, Pre: Pre intervention, S: Sessions, SDNN: Standard deviation of the NN intervals, RMSSD: Root mean square of successive differences between successive normal heartbeats, SDNN: Standard deviation of NN intervals, Mean RR: The average time between heartbeats in milliseconds, RMSSD: Root mean square of successive RR interval differences, PNN50: Percentage of successive RR intervals that differ by more than 50 ms, MXDMN: The difference between the maximum and minimum measured RR interval, MODA: Median of RR intervals.
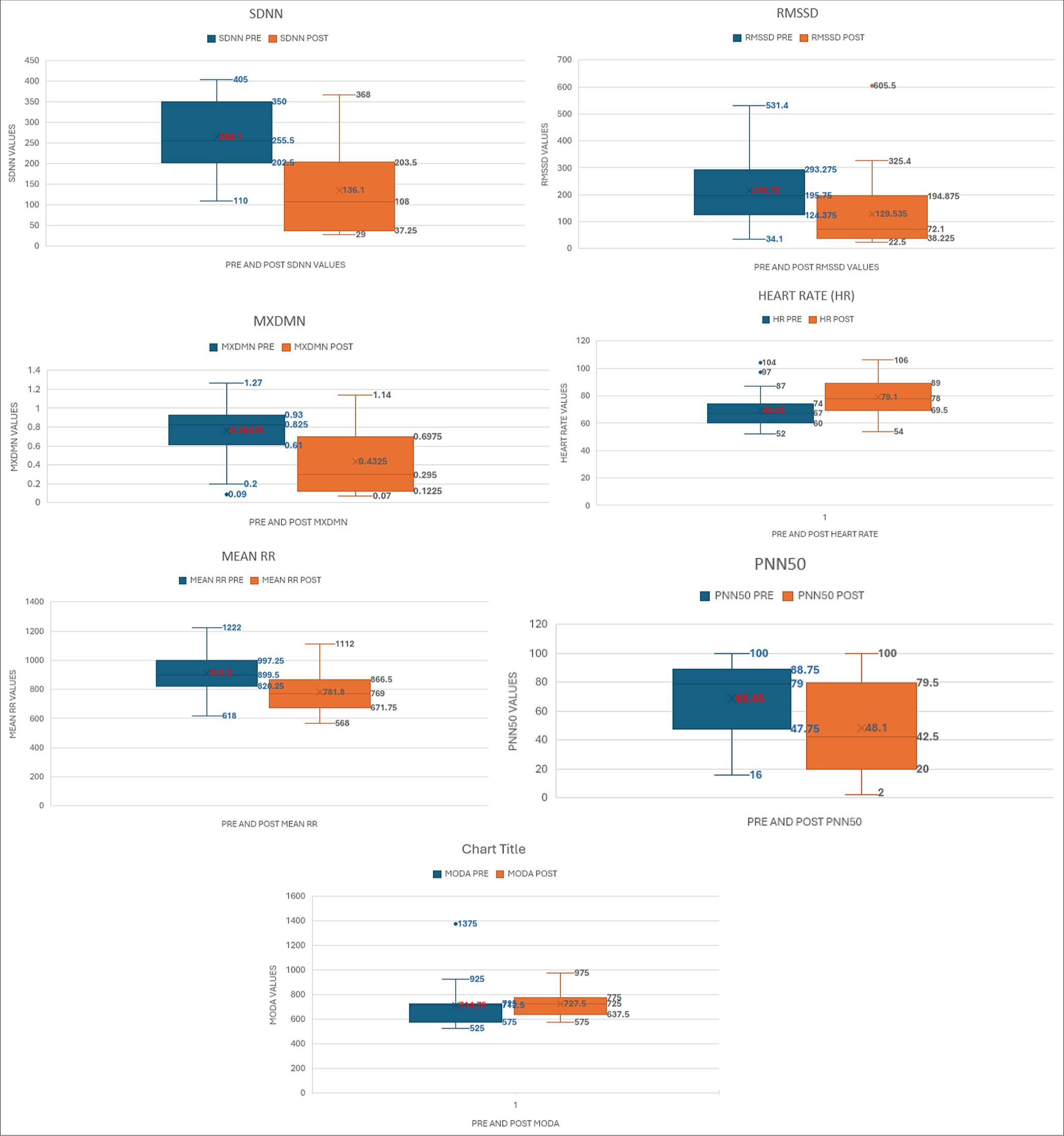
- Impact of yoga on heart rate variability parameters. SDNN: Standard deviation of the NN intervals, RMSSD: Root mean square of successive differences between successive normal heartbeats, MXDMN: The difference between the maximum and minimum measured RR interval, Mean RR: The average time between heartbeats in milliseconds, PNN50: Percentage of successive RR intervals that differ by more than 50 ms, MODA: Median of RR intervals.
Result of time domain of HRV in sports group
The initial SDNN (ms) value for the sports group was 202.20 ± 50.17(ms). Subsequent measurements at the 4th and 8th sessions indicated 98.90 ± 99.643 and 144.90 ± 139.63 (ms) values, respectively. SDNN (ms) values were reduced following the eighth session compared to the baseline data [Table 3 and Figure 3].
| Variables | Mean±SD | 95% confidence interval of the difference | T-statistic | Degree of freedom (df) | P-value | |
|---|---|---|---|---|---|---|
| Lower | Upper | |||||
| SDNN | ||||||
| PRE versus S4 | 202.20±50.177 | 52.34 | 154.25 | 4.24 | 19 | 0.09 |
| 98.90±99.643 | ||||||
| S4 versus S8 | 98.90±99.643 | −130.08 | 38.08 | −1.14 | 19 | 0.26 |
| 144.90±139.63 | ||||||
| PRE versus S8 | 202.20±50.177 | −10.34 | 124.94 | 1.77 | 19 | 0.09 |
| 144.90±139.63 | ||||||
| Mean RR | ||||||
| PRE versus S4 | 653.60±101.09 | −36.24 | 133.74 | 1.200 | 19 | 0.24 |
| 604.85±182.855 | ||||||
| S4 versus S8 | 604.85±182.855 | −61.99 | 175.09 | 0.998 | 19 | 0.33 |
| 658.55±135.585 | ||||||
| PRE versus S8 | 653.60±101.09 | −81.69 | 71.79 | −0.135 | 19 | 0.89 |
| 658.55±182.855 | ||||||
| RMSSD | ||||||
| PRE versus S4 | 67.30±49.59 | −65.72 | 65.82 | 0.002 | 19 | 0.99 |
| 67.25±118.60 | ||||||
| S4 versus S8 | 67.25±118.60 | −144.06 | 40.86 | −1.16 | 19 | 0.25 |
| 118.85±127.96 | ||||||
| PRE versus S8 | 67.30±49.59 | −100.99 | −2.101 | −2.18 | 19 | 0.04* |
| 118.85±127.96 | ||||||
| PNN50 | ||||||
| PRE versus S4 | 37.35±16.33 | 5.437 | 36.76 | 2.82 | 19 | 0.01* |
| 16.25±26.88 | ||||||
| S4 versus S8 | 16.25±6.88 | −38.801 | 5.601 | −1.56 | 19 | 0.13 |
| 32.85±31.86 | ||||||
| PRE versus S8 | 37.35±316.33 | −12.803 | 21.803 | 0.544 | 19 | 0.59 |
| 32.85±31.86 | ||||||
| MXDMN | ||||||
| PRE versus S4 | 0.200±0.41 | −18.95 | 5.95 | −1.09 | 19 | 0.28 |
| 6.70±26.80 | ||||||
| S4 versus S8 | 6.70±26.80 | −6.28 | 18.88 | 1.04 | 19 | 0.30 |
| 0.400±0.50 | ||||||
| PRE versus S8 | 0.200±0.41 | −0.52 | 0.125 | −1.28 | 19 | 0.21 |
| 0.400±0.50 | ||||||
| MODA | ||||||
| PRE versus S4 | 645.0±65.69 | 63.68 | 14108 | 5.50 | 19 | 0.00* |
| 542.25±61.37 | ||||||
| S4 versus S8 | 542.25±61.37 | −87.36 | 75026 | −0.15 | 19 | 0.87 |
| 548.30±174.85 | ||||||
| PRE versus S8 | 645.0±65.69 | 6.449 | 186.95 | 2.24 | 19 | 0.03* |
| 548.30±174.85 | ||||||
| HR | ||||||
| PRE versus S4 | 108.50±7.21 | −17.77 | 61.77 | 1.15 | 19 | 0.26 |
| 86.50±83.82 | ||||||
| S4 versus S8 | 86.50±83.82 | −47.753 | 28.353 | −0.53 | 19 | 0.60 |
| 96.20±21.41 | ||||||
| PRE versus S8 | 108.50±7.21 | 1.785 | 22.81 | 2.44 | 19 | 0.02* |
| 96.20±21.41 | ||||||
Bold and * indicates: Statistically significant at P<0.05, Pre: Pre intervention, S: Sessions, SDNN: Standard deviation of the NN intervals, RMSSD: Root mean square of successive differences between successive normal heartbeats, HR: Heart Rate, RR: The average time between heartbeats in milliseconds, RMSSD: Root mean square of successive RR interval differences, PNN50: Percentage of successive RR intervals that differ by more than 50 ms, MXDMN: The difference between the maximum and minimum measured RR interval, MODA: Median of RR intervals.

- Impact of sports on heart rate variability parameters. SDNN: Standard deviation of the NN intervals, RMSSD: Root mean square of successive differences between successive normal heartbeats, MXDMN: The difference between the maximum and minimum measured RR interval, Mean RR: The average time between heartbeats in milliseconds, PNN50: Percentage of successive RR intervals that differ by more than 50 ms, MODA: Median of RR intervals.
Comparison of yoga versus sports activities using HRV parameters
In the yoga intervention group, significant differences were observed across a range of parameters, including SDNN, mean RR interval, mean HR, RMSSD, the difference between the maximum and minimum measured RR interval (MxDMN), and pNN50, following the completion of the eight-session program. Notably, the yoga group demonstrated a statistically significant decrease in SDNN parameters after the eighth session compared to the baseline data. In contrast, the sports group exhibited no significant change in SDNN, mean RR interval, and MxDMN (P > 0.05) and increased RMSSD at the eight-session endpoint. Conversely, the yoga group significantly reduced RMSSD and MxDMN measurements (P < 0.05) compared to the sports group at the study period’s culmination [Table 4].
| Variables | Yoga (n=20) | Sports (n=20) | ||||
|---|---|---|---|---|---|---|
| Pre-intervention | Post-intervention | P-value | Pre-intervention | Post-intervention | P-value | |
| SDNN | 266.10±85.99 | 136.10±111.83 | 0.00* | 202.20±50.177 | 144.90±139.63 | 0.09 |
| Mean RR | 913.30±150.69 | 781.80±139.29 | 0.00* | 653.60±101.09 | 658.55±165.58 | 0.89 |
| RMSSD | 216.75±131.135 | 129.50±141.858 | 0.01* | 67.30±49.59 | 118.85±127.96 | 0.04* |
| PNN50 | 68.85±24.51 | 48.10±32.14 | 0.01* | 37.35±16.33 | 32.85±31.86 | 0.59 |
| MXDMN | 0.85±0.36 | 0.40±0.50 | 0.00* | 0.200±0.410 | 0.400±0.502 | 0.21 |
| MODA | 714.75±185.09 | 727.50±108.185 | 0.79 | 645.00±65.69 | 548.30±174.85 | 0.03* |
| Heart rate | 69.55±79.10 | 79.10±13.52 | 0.00* | 108.50±7.21 | 96.20±21.41 | 0.02* |
Comparison of yoga versus sports activities using Depression Anxiety Stress Scales (DASS)-42 questionnaire
The DAS-42 score ranges from 0 to 126 points, indicating typical and mild symptoms at 0–32, severe symptoms at 33–39, and extreme severity at 50 and above. In the yoga group, the pre- and post-session DAS-42 scores were 47.6 ± 32.1 and 29.7 ± 27.8 (P < 0.05), respectively, while in the sports group, the scores were 44.0 ± 12.1 and 38.5 ± 16.5, for pre- and post-session, (P > 0.05), respectively [Table 5].
| Variables | Yoga (n=20) | Sports (n=20) | ||||
|---|---|---|---|---|---|---|
| Pre | Post | P-value | Pre | Post | P-value | |
| DASS-42 score | 47.6±32.1 | 29.7±27.8 | 0.00 | 44.0±12.1 | 38.5±16.5 | 0.08 |
DASS: Depression, Anxiety, and Stress Scale, Bold value: Statistically significant at P<0.05
DISCUSSION
This study significantly contributes to the literature by assessing the effects of traditional and contemporary exercise methods on HRV, an area that remains underexplored. The findings reveal that no statistically significant differences were observed in the SDNN or the RMSSD in sports activity. In contrast, significant alterations were observed in the SDNN, mean RR interval, mean HR, RMSSD, MxDMN, and pNN50 among the participants who practiced yoga. After yoga practice, a marginal increase in HR was evident. Decreased overall HRV (SDNN) following the practice indicates a positive health outcome. Following a yoga session, pNN50 was significantly reduced, indicating an enhancement in the adaptability of the ANS. This improvement is associated with increased cardiovascular fitness, lower stress levels, and a comprehensive enhancement in overall health.
In addition, the decrease in RMSSD and MxDMN measurements reflects an adaptive response of the cardiovascular systems to external stressors, indicating flexible autonomic regulation and effective vagal activity. This adaptation may be attributed to heightened vagal tone or sympathetic withdrawal after implementing yoga practices. Ultimately, these results imply that participants in the yoga group manifested heightened parasympathetic tone following yoga therapy compared to their counterparts in the sports group.
Following sports participation, HRV reflects sympathetic dominance during physical activity to address heightened oxygen and nutrient requirements. After exercising, parasympathetic activity increases as the body recovers. In conclusion, changes in HRV metrics after physical exertion indicates a shift from effort to recovery. This highlights a more balanced autonomic state led by the parasympathetic nervous system as the body seeks to regain equilibrium.
The yoga and sports groups exhibited increased HR, indicating sympathetic activation and muscle exertion. These findings align with those of Bhavanani et al.,[16] who similarly documented increased HR pre- and post-repetitive yoga practices. SDNN, an indicator of overall HRV, was notably changed during Yoga, corroborating the observations of Malhotra et al.,[17] who noted significant changes in SDNN following yoga practice. The ANS effectively manages stress after repeated yoga sessions, as indicated by reduced SDNN values in the yoga group. This aligns with Farinatti et al.,[18] who found decreased SDNN post-exercise due to combined parasympathetic and sympathetic modulations. Furthermore, the decrease in RMSSD and MxDMN measurements after yoga corresponds to similar results observed in an interventional study conducted by Pal et al.[19] in Puducherry, India, where cardiovascular autonomic functions of apparently healthy, male medical students were assessed following a short-term relaxation therapy regimen. The results demonstrated an improvement in autonomic balance toward parasympathetic activity after a short-term practice of relaxation therapy.
Similar studies have been reported by An et al.,[20] Patra and Telles,[21] and Vempati and Telles[22] which have demonstrated that yoga-based guided relaxation techniques, such as cyclic meditation and Shavasana, can modulate HRVs in a parasympathetic manner. A study done by Naswa et al. suggests that the inclusion of Rajyoga meditation along with conventionally given cardiac rehabilitation enhanced metabolic resilience with lowered resting metabolism and enhanced recovery post-surgery in children operated on for congenital heart disease. There was an improvement in the psychological adjustment and behavior of adolescents.[23]
Limitations
The interpretation of HRV changes is intricate and can be affected by factors such as individual characteristics, consistency of practice, and overall health. Therefore, for a thorough assessment, it is advisable to monitor HRV over a prolonged period and consider other physiological and subjective well-being indicators. In addition, increasing the sample size and ensuring random distribution of subjects would be beneficial.
CONCLUSION
The study observed a significant improvement in cardiac autonomic function, indicating that yoga positively impacts an individual’s overall health status. These effects were notably evident after a short duration of yoga practice. Long-term engagement in yoga could mitigate the risk of physiological and psychological ailments and enhance overall quality of life. Yoga is a non-pharmacological treatment strategy for individuals experiencing stress. However, the sports intervention improved the body’s ability to manage stress. At the same time, yoga therapy resulted in a heightened parasympathetic tone compared to the sports intervention.
Ethical approval
The research/study approved by the Institutional Ethical Committee at ACS Medical College and Hospital, number 956/2023/IEC/ACSMCH, dated 17th November 2023.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
Financial support and sponsorship: Nil.
References
- Academic Achievement Motivation and School Satisfaction among Adolescents. Int J Indian Psychol. 2023;11:1494-528.
- [Google Scholar]
- Factors Influencing the Students Academic Performance in Secondary Schools in India Germany: Research Gate; 2018.
- [Google Scholar]
- Stress and its Effects on Medical Students: A Cross-sectional Study at a College of Medicine in Saudi Arabia. J Health Popul Nutr. 2011;29:516-22.
- [CrossRef] [PubMed] [Google Scholar]
- Medical Students' Perceptions of Stress Due to Academic Studies and Its Interrelationships with Other Domains of Life: A Qualitative Study. Med Educ Online. 2019;24:1603526.
- [CrossRef] [PubMed] [Google Scholar]
- Job Demand-Control-Support Latent Profiles and their Relationships with Interpersonal Stressors, Job Burnout, and Intrinsic Work Motivation. Int J Environ Res Public Health. 2020;17:9430.
- [CrossRef] [PubMed] [Google Scholar]
- Cognitive, Emotional, Physical, and Behavioral Stress-related Symptoms and Coping Strategies among University Students during the Third Wave of COVID-19 Pandemic. Front Psychiatry. 2022;13:933981.
- [CrossRef] [PubMed] [Google Scholar]
- Trend Analysis of Cardiovascular Disease Mortality, Incidence, and Mortality-to-incidence Ratio: Results from Global Burden of Disease Study 2017. BMC Public Health. 2021;21:401.
- [CrossRef] [PubMed] [Google Scholar]
- Autonomic Nervous System Dysfunction: JACC Focus Seminar. J Am Coll Cardiol. 2019;73:1189-206.
- [CrossRef] [PubMed] [Google Scholar]
- Autonomic Imbalance, Hypertension, and Cardiovascular Risk. Am J Hypertens. 2000;13:112S-22.
- [CrossRef] [PubMed] [Google Scholar]
- The Role of Heart Rate Variability (HRV) in Different Hypertensive Syndromes. Diagnostics (Basel). 2023;13:785.
- [CrossRef] [PubMed] [Google Scholar]
- Novel Approaches to Restore Parasympathetic Activity to the Heart in Cardiorespiratory Diseases. Am J Physiol Heart Circ Physiol. 2020;319:H1153-61.
- [CrossRef] [PubMed] [Google Scholar]
- Yoga and Heart Rate Variability: A Comprehensive Review of the Literature. Int J Yoga. 2016;9:97-113.
- [CrossRef] [PubMed] [Google Scholar]
- Factors Affecting Training and Physical Performance in Recreational Endurance Runners. Sports (Basel). 2020;8:35.
- [CrossRef] [PubMed] [Google Scholar]
- Validity and Reliability of Different Smartphones Applications to Measure HRV During Short and Ultra-Short Measurements in Elite Athletes. Comput Methods Programs Biomed. 2022;217:106696.
- [CrossRef] [PubMed] [Google Scholar]
- Manual for the Depression Anxiety Stress Scales. 1995 Available from: https://www2.psy.unsw.edu.au/groups/dass [Last accessed 2025 Jan 02]
- [CrossRef] [Google Scholar]
- Immediate Effects of Suryanamaskar on Reaction Time and Heart Rate in Female Volunteers. Indian J Physiol Pharmacol. 2013;57:199-204.
- [Google Scholar]
- Heart rate Variability among Healthy Untrained Adults During Mild Intensity Stationary Cycling Exercise. Adv Biomed Res. 2023;12:55.
- [CrossRef] [PubMed] [Google Scholar]
- Acute Effects of Stretching Exercise on the Heart Rate Variability in Subjects with Low Flexibility levels. J Strength Cond Res. 2011;25:1579-85.
- [CrossRef] [PubMed] [Google Scholar]
- The Effects of Short-term Relaxation Therapy on Indices of Heart Rate Variability and Blood Pressure in Young Adults. Am J Health Promot. 2014;29:23-8.
- [CrossRef] [PubMed] [Google Scholar]
- Measures of Heart Rate Variability in Women Following a Meditation Technique. Int J Yoga. 2010;3:6-9.
- [CrossRef] [PubMed] [Google Scholar]
- Heart Rate Variability during Sleep Following the Practice of Cyclic Meditation and Supine Rest. Appl Psychophysiol Biofeedback. 2010;35:135-40.
- [CrossRef] [PubMed] [Google Scholar]
- Yoga-Based Guided Relaxation Reduces Sympathetic Activity Judged from Baseline Levels. Psychol Rep. 2002;90:487-94.
- [CrossRef] [PubMed] [Google Scholar]
- Randomized Control Study to Evaluate the Effect of Rajyoga Meditation on Metabolic and Psychological Correlates of Health in Patients of Surgical Repair for Congenital Heart Disease. J Card Crit Care TSS. 2024;8:217-22.
- [CrossRef] [Google Scholar]




