
Translate this page into:
Mycotic Pseudoaneurysm of the Ascending Aorta following Coronary Artery Bypass Graft Surgery
*Corresponding author: Ajmer Singh, Department of Cardiac Anaesthesia, Medanta The Medicity, Gurugram, Haryana, India. ajmersingh@yahoo.com
-
Received: ,
Accepted: ,
How to cite this article: Singh A, Mukati R, Mehta Y. Mycotic Pseudoaneurysm of the Ascending Aorta following Coronary Artery Bypass Graft Surgery. J Card Crit Care TSS. 2024;8:226-9. doi: 10.25259/JCCC_20_2024
Abstract
Formation of ascending aortic mycotic pseudoaneurysm after cardiac surgery is an uncommon complication associated with high mortality. A 69-year-old male presented with complaints of intermittent fever and chest pain 6 weeks after coronary artery bypass graft surgery. Echocardiography and computed tomography angiography of the chest revealed a large pseudoaneurysm communicating with the distal ascending aorta. The surgical procedure, consisting of cleaning and excision of the pseudoaneurysm followed by the closure of the neck of the aneurysm with a pericardial patch, performed under deep hypothermic circulatory arrest, led to a favorable outcome.
Keywords
Mycotic aneurysm
Ascending aorta
Deep hypothermic circulatory arrest
Coronary artery bypass graft surgery

INTRODUCTION
Pseudoaneurysm of the thoracic aorta is an uncommon complication after cardiac surgery, with a reported incidence of about 0.65–2%.[1] Mycotic pseudoaneurysm can result from secondary infection caused by bacterial endocarditis and mediastinitis. It can develop by infection at a previous aortotomy or aortic cannulation site several weeks, months, or up to 3 years after cardiac surgery.[2] Conservative management is associated with high mortality rates of about 88–95%, while surgical reconstruction of the aorta has reduced the mortality to about 25%.[3] Possible sites of aortic pseudoaneurysm formation after cardiac surgery include aortotomy site, clamping site, partial side-biting clamp site, proximal graft anastomosis site, cardioplegia needle site, and cannulation site. Here, we describe a patient who developed a large ascending aortic mycotic pseudoaneurysm 6 weeks after coronary artery bypass graft (CABG) surgery and required surgical repair under deep hypothermic circulatory arrest (DHCA).
CASE REPORT
A 69-year-old man with type II diabetes mellitus was referred to our institution for evaluation of intermittent high-grade fever and chest pain. He had undergone an off-pump multi-vessel CABG 6 weeks ago and was treated conservatively with intravenous antibiotic therapy without any relief. Physical examination showed a wound with pus discharge from the upper part of the sternum. Streptococcus pyogenes was isolated from the pus culture, which was sensitive to vancomycin and ceftazidime; and appropriate antibiotic therapy was initiated. The blood culture was sterile. A transthoracic echocardiography showed a pseudoaneurysm of the anterior wall of the distal ascending aorta with normal valves and ventricular function. Computed tomography (CT) angiography of the chest also showed a large, saccular shaped, pseudoaneurysm measuring 40 mm × 30 mm, communicating with the ascending aorta [Figure 1]. Surgical repair of the pseudoaneurysm was planned. Intraoperative transesophageal echocardiography confirmed the CT findings [Figure 2]. Following systemic heparinization, right axillary artery and femoral venous cannulations were done for cardiopulmonary bypass (CPB). Sternotomy was done after the institution of CPB given the proximity of the aneurysm to the sternum. The patient was cooled to 18°C temperature, and DHCA with unilateral antigrade cerebral perfusion was started at a flow rate of 500 mL/min under cerebral oximetry monitoring. For cerebral protection, methylprednisolone, mannitol, and topical head cooling were used. After careful dissection, local wound debridement, and clearing of the clots, a pseudoaneurysm was identified just distal to the proximal anastomosis of the vein graft [Figure 3]. The ostia of venous grafts were patent. The neck of the pseudoaneurysm was identified and closed using a glutaraldehyde-treated bovine pericardial patch. The duration of DHCA and CPB was 32 min and 166 min, respectively. Weaning from CPB and further course of the patient in the hospital were uneventful.
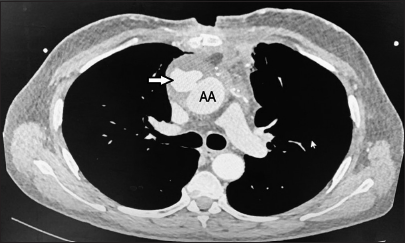
- Computed tomography angiography axial section showing a large, saccular pseudoaneurysm (arrow) communicating with the ascending aorta (AA).
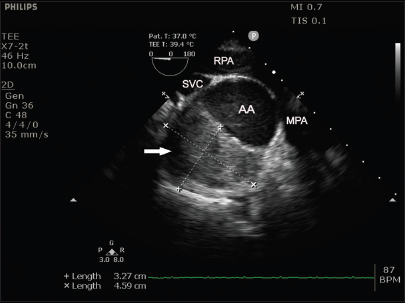
- Intraoperative transesophageal echocardiography ascending aorta short-axis view showing aortic pseudoaneurysm filled with blood-clots (arrow) communicating with the ascending aorta (AA). SVC: Superior vena cava, RPA: Right pulmonary artery, MPA: Main pulmonary artery.
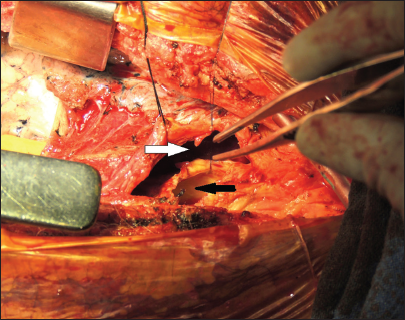
- Photograph taken during surgery after removal of the clots from the pseudoaneurysm cavity (white arrow) and opened anterior wall of the ascending aorta (black arrow).
DISCUSSION
Mycotic pseudoaneurysm of the aorta is a rapidly growing, localized, and abnormal dilatation of its wall that develops secondary to an infection. It is triggered by intimal damage, inflammation, and bacterial infiltration of the wall of the aorta. It should be suspected in patients with unexplained fever who have undergone any interventional or surgical procedure of the cardiovascular system. Predisposing factors for pseudoaneurysm of the ascending aorta include prior aortic dissection, uncontrolled hypertension, infection, immunosuppression, connective tissue disorders, and aortic manipulation during surgery.[4] The pathophysiology involves an amalgamation of arterial injury, bacterial spreading, intimal infection, and release of proinflammatory cytokines leading to focal breakdown of the vessel wall and aneurysm formation. Anatomically, mycotic pseudoaneurysm of the aorta is least commonly located in the ascending aorta (0.7%) in contrast to the arch or descending aorta (23.6% and 75.7%, respectively).[5]
The patients with mycotic pseudoaneurysm of the aorta require urgent surgical intervention due to the risk of impending rupture, which carries high mortality. Mycotic aneurysms grow rapidly, several centimeters per month, in contrast to non-mycotic aneurysms which progress about 0.3–0.6 cm/year.[6] Compared to a percutaneous exclusion of the aneurysm, surgery is more appropriate in cases with mediastinal infection, hemodynamic instability, or impending rupture. Furthermore, in this patient, the distal part of the aneurysm was in close proximity to the arch vessels and thus not suitable for endovascular treatment. A large multicenter European study consisting of 123 patients has shown that mycotic pseudoaneurysm can be treated by endovascular technique, but late infection-related complications can occur and often lead to high mortality.[7] Endovascular therapy could be used either as a palliative therapeutic choice in select patients, or as a bridge to elective surgery, after recovery from the initial emergency. Adhesions from the previous surgery can complicate the surgical management of this condition, and there is the risk of exsanguination during resternotomy. Massive bleeding at the time of re-sternotomy resulting from rupture of the aneurysmal sac requiring emergency cannulation for CPB has been reported. Patients with anteriorly located aneurysms, aneurysm size measuring more than 55 mm, and those eroding into the outer sternum are at a higher risk of rupture and hemorrhage.[8] Initiation of CPB before sternotomy is a well-known strategy to prevent this fatal complication. The integral part of the procedure was the safe institution of CPB and the desired level of hypothermia to achieve neuroprotection. Cannulation of the carotid artery for CPB and femorofemoral bypass with moderate hypothermia and transient circulatory arrest has also been reported.[9]
Most definitive therapy for a mycotic aneurysm involves the replacement of the ascending aorta with a homograft, which is a time-consuming and more complex procedure. If the neck of the pseudoaneurysm is small and the surrounding aorta is not involved, as observed in this patient, the pseudo-aneurysm may be repaired with a patch. The use of a biological material has shown superior results compared to a synthetic material such as Dacron patch, which is more prone to bacterial seeding and risk of reinfection.[10] A conservative technique to treat mycotic aneurysms, however, cannot prevent further dilatation of the aortic wall as the adult aorta cannot resynthesize the damaged elastin fibers.
Methods to prevent post-operative mediastinal pseudoaneurysms have been emphasized, such as performing precise aortic suture techniques, vigilant handling of the aorta wall, meticulous asepsis, and aggressive treatment of perioperative infection. Among the causative organisms isolated from cultures after surgery for mycotic aneurysms, Staphylococcus species (34.1%) and Streptococcus species (23.2%) are the most common.[11-13] For patients with extensive sternal osteomyelitis, rigorous surgical treatment with thorough wound cleaning, plastic reconstruction, bone removal, and mediastinal irrigation with disinfectant in combination with intravenous antibiotic therapy may be required. We could not isolate any organism from the culture of the surgical specimen, probably due to the antimicrobial therapy received by the patient. We presume that the patient described here developed bacteremia after CABG, which led to mycotic pseudoaneurysm formation.
CONCLUSION
Although mycotic pseudoaneurysm formation following cardiac surgery is rare, prompt diagnosis and timely surgical intervention can avoid the associated catastrophic complications and reduce mortality.
Ethical approval
The Institutional Review Board approval is not required.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Conflicts of interest
Dr. Yatin Mehta is on the editorial board of the Journal.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
Financial support and sponsorship
Nil.
References
- Management of Infected Aortoiliac Aneurysms. Arch Surg. 1991;126:873-8. discussion 878-9
- [CrossRef] [Google Scholar]
- Mycotic Ascending Aortic Pseudoaneurysm at Aortic Cannulation Site. Asian Cardiovasc Thorac Ann. 2009;17:417-8.
- [CrossRef] [Google Scholar]
- Surgical Mortality in Patients with Infected Aortic Aneurysms. J Am Coll Surg. 2003;196:435-41.
- [CrossRef] [Google Scholar]
- Infected Aortic Aneurysms: Aggressive Presentation, Complicated Early Outcome, but Durable Results. J Vasc Surg. 2001;34:900-8.
- [CrossRef] [Google Scholar]
- Nationwide Study on Treatment of Mycotic Thoracic Aortic Aneurysms. Eur J Vasc Endovasc Surg. 2019;57:239-46.
- [CrossRef] [Google Scholar]
- The Natural History of Thoracic Aortic Aneurysms. J Thorac Cardiovasc Surg. 1994;107:1323-33. discussion 1332-3
- [CrossRef] [Google Scholar]
- Endovascular Treatment of Mycotic Aortic Aneurysms: A European Multicenter Study. Circulation. 2014;130:2136-42.
- [CrossRef] [Google Scholar]
- Surgical Management of a Giant Ascending Aortic Pseudoaneurysm. Tex Heart Inst J. 2010;37:710-3.
- [Google Scholar]
- Surgery for Pseudoaneurysm of the Ascending Aorta Under Moderate Hypothermia. J Cardiothorac Surg. 2011;6:125.
- [CrossRef] [Google Scholar]
- Mycotic Aneurysm in a Child with History of Coarctation of the Aorta Repair. Ann Pediatr Cardiol. 2014;7:138-41.
- [CrossRef] [Google Scholar]
- Aortic Root Pseudoaneurysm: A Case Report and Literature Review. Indian J Thorac Cardiovasc Surg. 2024;40:68-77.
- [CrossRef] [Google Scholar]
- The Importance of TEE Examination in Patients with Pseudoaneurysm of Arch of Aorta Post-TEVAR Procedure. J Card Crit Care TSS. 2022;6:173-6.
- [CrossRef] [Google Scholar]
- Left Ventricular Contained Rupture: True or Pseudoaneurysm? J Card Crit Care TSS. 2017;1:40-4.
- [CrossRef] [Google Scholar]




