
Translate this page into:
Femoral Nerve Block for Emergency Femoral Artery Saddle Embolectomy
*Corresponding author: Sambhunath Das, Department of Cardiac Anaesthesia and Critical Care, AIIMS Hospital, New Delhi, India. sambhunathds833@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Singh R, Das S. Femoral nerve block for emergency femoral artery saddle embolectomy. J Card Crit Care TSS 2023;7:111-2.
A 38-year-old female was diagnosed with a case of severe mitral stenosis with atrial fibrillation and with a left atrial (LA) clot. The patient was admitted for mitral valve replacement and LA clot removal. In the pre-operative period, the patient suddenly complained of weakness and coldness in both the lower limbs. Arterial and Venous Doppler revealed acute thrombosis of abdominal aorta after the origin of the inferior mesenteric artery extending into bilateral common iliac artery with monophasic flow [Figure 1] in bilateral common femoral artery, superficial femoral artery, and popliteal artery. Diagnosis of acute limb ischemia was confirmed and patient was posted for emergency saddle thrombectomy. In view of acute vascular ischemia and paraparesis and severe pain, femoral embolectomy was planned under regional anesthesia in the form of an ultrasound-guided femoral nerve block. Anti-aspiration prophylaxis was administered to the patient. Her prothrombin time and international normalized ratio were 20 s was 1.6, respectively.

- Schematic diagram of monophasic Doppler flow pattern due to femoral artery embolus.
The procedure for the femoral nerve block was explained to the patient in her language. Bilateral inguinal regions were painted with betadine and covered with sterile drapes. M turbo Sonosite machine with a linear probe of frequency of 5–10 MHz was selected for visualization of femoral nerve anatomy. Probe was placed just below the inguinal crease and the femoral vein, artery, and nerve bundle were appreciated from medial to lateral [Figure 2]. Once the femoral nerve bundle was localized, a block needle was inserted using in plain approach. The needle tip was visualized in the femoral nerve bundle, after that hydro dissection was achieved with 1–2 mL of saline. Fifteen mL of 0.375% ropivacaine was injected into the femoral nerve plain. The same procedure of nerve block was repeated on the other side. After 10–15 min, surgery was started. The patient did not complain of any pain during the procedure. Hemodynamic parameters were stable throughout the procedure. The total operative time was 1.5 h. Immediately following the embolectomy, her limbs became warm and distal pulsation became palpable with normal biphasic flow [Figure 3]. The patient was shifted to the recovery area. There were no signs of residual motor weakness in the lower limbs.

- Ultra sonographic image of femoral nerve block. V: Femoral vein, A: Femoral artery, N: Femoral nerve.

- Ultra sonographic image of biphasic flow pattern of normal blood flow in femoral artery after embolectomy.
The dislodgment and migration of LA clots to abdominal, femoral, and peripheral arteries including stroke is an emergency.[1] Immediate embolectomy is life-saving by re-establishing perfusion. Femoral nerve [Figure 4] block anesthesia is a possible technique for embolectomy from the femoral artery approach.[2] It will avoid the use of general anesthesia and neurological assessment can be performed during embolectomy. The patient will have complete analgesia, quick mobility, and vasodilatation effect due to sympathetic nerve block compared to GA. Hence, monitored anesthesia care with bilateral femoral nerve block is an alternative method of anesthesia for saddle embolectomy.
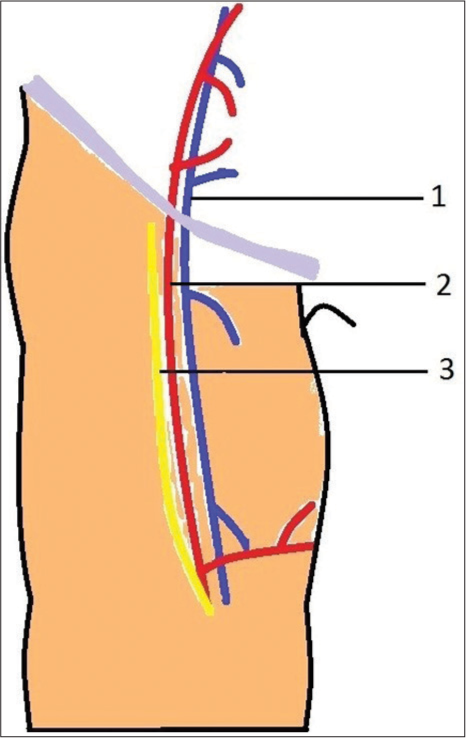
- Anatomical relationship of femoral vein, and femoral nerve at the groin. (1: Femoral Vein, 2: Femoral Artery and 3: Femoral Nerve).
Declaration of patient consent
Patient’s consent not required as there are no patients in this study.
Conflicts of interest
There are no conflicts of interest.
Financial support and sponsorship
Nil.
References
- Diagnosis and treatment of aortic saddle embolism. Ann Vasc Surg. 2018;56:124-31.
- [CrossRef] [PubMed] [Google Scholar]




