
Translate this page into:
Transesophageal Echocardiography of Mitral Valve Repair in a Case of Sinus of Valsalva Aneurysm: 2D versus 3D
Neeti Makhija, MD Room No. 9, 7th Floor, Department of Cardiac Anaesthesia and Critical Care, Cardiothoracic Centre, All India Institute of Medical Sciences New Delhi, Ansari Nagar, New Delhi 110029 India neetimakhija@hotmail.com
This article was originally published by Thieme Medical and Scientific Publishers Pvt. Ltd. and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Mitral valve repair is a common and preferred technique over mitral valve replacement whenever it is feasible. Transesophageal echocardiography (TEE) not only reliably identify repairable mitral valve but also guide appropriate intervention. In addition to two-dimensional (2D) TEE, the three-dimensional (3D) technique clearly delineates size and shape of mitral valve apparatus, and determine the repairability and success of repair technique. We illustrate the 2D and 3D TEE techniques that guided the surgical intervention for Alfieri repair.
Keywords
2D echocardiography
3D echocardiography
Alfieri stitch
mitral valve repair
sinus of Valsalva repair
transesophageal echocardiography

Mitral valve repair is a common and preferred technique over mitral valve replacement whenever it is feasible. Transesophageal echocardiography (TEE) not only reliably identify repairable mitral valve but also guide appropriate intervention. In addition to two-dimensional (2D) TEE, the three-dimensional (3D) technique clearly delineates size and shape of mitral valve apparatus, determine repairability and success of repair technique. We illustrate the 2D and 3D TEE techniques that guided the surgical intervention for Alfieri repair.
A 49-year-old hypertensive woman was admitted to the hospital with shortness of breath for 3 months. She had sudden onset of breathlessness and chest pain radiating to the back, which relieved on taking rest. She had raised urea and creatinine level, for which nephrology consultation was done.
Transthoracic echocardiography revealed non-coaptation of aortic valve, sinus of Valsalva (SOV) aneurysm with right coronary cusp prolapsed, severe aortic regurgitation with holodiastolic flow reversal in descending thoracic aorta (DTA), enlarged left ventricle, moderate mitral regurgitation. Contrast-enhanced computed tomography revealed mild cardiomegaly with suspected mild focal dilatation of the right coronary cusp of aortic sinus. Medical management with diuretics and vasodilators was instituted. She had raised urea and creatinine level therefore, nephrology opinion, and optimization was done prior to planning for aortic valve replacement (AVR) with SOV aneurysm repair.
The patient was taken to operation theater for surgical intervention. All ASA monitors attached, large bore venous access, and left radial arterial line were secured. Balanced anesthesia technique was used for induction with injection fentanyl, midazolam, etomidate, and intubation facilitated with muscle relaxant rocuronium. Patient's hemodynamics was well maintained during intraoperative period. A triple-lumen central venous catheter was inserted in the right internal jugular vein and TEE probe was placed.
TEE was performed using an X7–2t Philips's ultrasound probe and machine (iE33 model; Philips, Bothell, WA, USA). TEE revealed dilated right SOV in the mid esophageal aortic valve short axis view (Fig. 1) and in the mid-esophageal long axis view (Fig. 2) (Video 1). On color Doppler interrogation, moderate-to-severe aortic regurgitation (Video 2) was noted having vena contracta 0.52 cm (Fig. 3A), pressure half time 274 ms (Fig. 3B), jet width to LVOT width around 0.6 (Fig. 3C), and holodiastolic flow reversal in the DTA (Fig. 3D). Moderate mitral regurgitation with central jet having vena contracta 0.42 cm (Fig. 4A) was found. Repairability criteria was met, with anterior mitral leaflet length 2.54 cm, (Fig. 4B) C-sept distance 3.9 cm, coaptation distance 1.5 cm, and coaptation area 2.94 cm2 (Fig. 4C), and posterior mitral leaflet length 1.3 cm (Fig. 4D). Cardiopulmonary bypass (CPB) was instituted after adequate heparinization. Sinus of Valsalva aneurysm was repaired with trans aortic Gortex patch and aortic valve replacement done with a #21 mm St Jude valve. Aortic cross clamp was released after 76 minutes. With the support of dobutamine 5 µg/kg/min, and nitroglycerin 0.5 µg/kg/min CPB was weaned. Post CPB, TEE done, which revealed increased severity of mitral regurgitation with vena contracta of 0.52 cm (Fig. 5). Therefore, it was planned to go on CPB again for mitral valve repair. Mitral valve repair was performed by Alfieri technique. After 22 minutes, aortic cross clamp was released. TEE was done again, which revealed adequate size double orifice mitral valve (Fig. 6) (Video 3). After protamine neutralization and adequate hemostasis patient shifted to the ICU after the surgery for further postoperative management. After 6 hours of mechanical ventilation, the patient was extubated and the patient was discharged after 5 days.
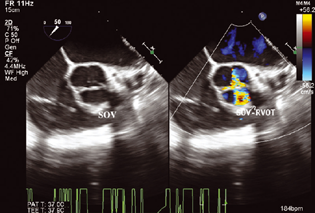
- Mid-esophageal aortic valve (AoV) short axis view with color comparison showing tricuspid AoV and aneurysmal dilatation of the right coronary sinus of Valsalva (SOV).
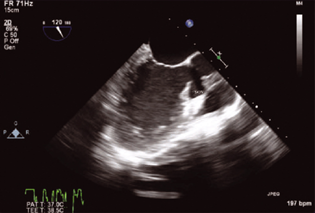
- Mid-esophageal long axis view illustrating asymmetric dilatation of the right coronary sinus of Valsalva (SOV).
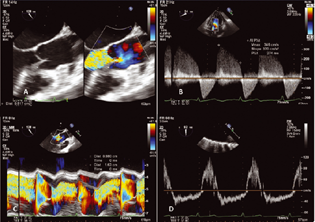
- Demonstration of severe aortic regurgitation: Mid-esophageal aortic valve (AoV) long axis view with color comparison showing vena contracta 0.52 cm (A), Continuous wave Doppler interrogation across aortic valve in the deep transgastric view, revealing a pressure half time of 274 ms (B), colored M- mode in the mid-esophageal aortic valve (AoV) long axis view measuring jet width to LVOT width ratio of around 0.6 (C), and holodiastolic flow reversal noted on pulse wave Doppler interrogation in the descending thoracic aorta (D).
- Demonstration of moderate mitral regurgitation: mid-esophageal four-chamber view with color Doppler interrogation showing a central regurgitant jet having vena contracta 0.42 cm (A). Mid-esophageal long axis view illustrating the anterior mitral leaflet length 2.54 cm, (B) C-sept distance 3.9 cm, tenting height 1.5 cm and tenting area 2.94 cm,2 (C) and posterior mitral leaflet length of 1.3 cm (D).
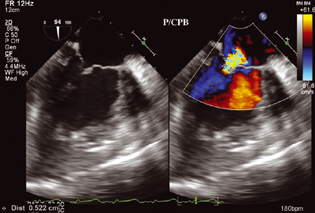
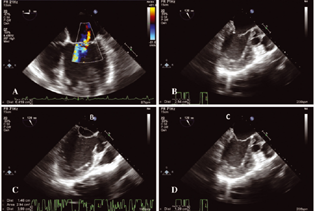
- Post cardiopulmonary bypass (P/CPB) mid-esophageal four-chamber view with color Doppler interrogation demonstrating a central regurgitant jet having vena contracta 0.52 cm.

- Three-dimensional mitral enface view (zoomed) illustrating double-orifice mitral valve after edge-to-edge MV repair, i.e., Alfieri stitch.

The edge-to-edge MV repair (i.e., Alfieri stitch) can pose a unique challenge in assessing iatrogenic mitral stenosis (MS). The Alfieri stitch was introduced in the 1990s to repair mitral valve (MV) with complex pathology.1 This technique relies on the precise identification of the regurgitant jet and area of leaflet coaptation and requires suture placement to approximate the free edges at the specific site of malcoaptation, resulting in a double-orifice MV inflow. The two created orifices may have relatively the same or different sizes depending on the site of suture placement along the leaflet coaptation line.2, 3 Intraoperatively, TEE plays a vital role in guiding the surgical technique and determine the success of repair technique.4 The use of two-dimensional and the three-dimensional TEE technique clearly delineate size and shape of double-orifice MV inflow and the adequacy of flow across it.5
Conflict of Interest
None declared.
References
- The double-orifice technique in mitral valve repair: a simple solution for complex problems. J Thorac Cardiovasc Surg. 2001;122(4):674-681.
- [Google Scholar]
- Asymmetric Alfieri's stitch to correct systolic anterior motion after mitral valve repair. Eur J Cardiothorac Surg. 2011;39(5):779-781.
- [Google Scholar]
- Edge-to-edge repair for prevention and treatment of mitral valve systolic anterior motion. J Thorac Cardiovasc Surg. 2013;146(4):836-840.
- [Google Scholar]
- Transesophageal echocardiography of the edge-to-edge technique of mitral valve repair. Anesth Analg. 2007;105(5):1231-1232.
- [Google Scholar]
- The hemodynamic effects of double-orifice valve repair for mitral regurgitation: a 3D computational model. Eur J Cardiothorac Surg. 1999;15(4):419-425.
- [Google Scholar]




