
Translate this page into:
Inadvertent Radial Artery Avulsion during Coronary Artery Angiography
Chinmaya Nanda, MD, FIACTA Medanta Institute of Critical Care and Anaesthesiology, Medanta The Medicity Sector 38, Gurgaon, 122001 India nandachinu@gmail.com
This article was originally published by Thieme Medical and Scientific Publishers Pvt. Ltd. and was migrated to Scientific Scholar after the change of Publisher.
A 53-year-old man was admitted to the hospital with complaints of dyspnea on exertion (grade 3). His resting echo showed no left ventricular regional wall motion abnormalities, with an ejection fraction of 55%, normal right ventricular function, and mild tricuspid regurgitation. His treadmill test was mildly positive. In view of a strong family history of coronary artery disease, he was planned for a coronary angiography.
The patient underwent coronary angiography, which was performed through right radial artery catheterization using a 5-Fr Tiger catheter. Coronary angiogram showed noncritical coronary artery disease. After the angiography was over, there was resistance on pulling out the catheter and guidewire. On excessive manipulation to take out the guidewire and catheter, the catheter was sheared and the guidewire could not be taken out. After sometime, the right hand became cold and the pulse was absent distal to the puncture site. Vascular surgery consultation was taken and the patient was planned for emergency surgical exploration to remove the retained radial artery catheter (Fig. 1). Tip of the 5-Fr catheter was found to be outside the lumen of the radial artery in the subcutaneous plane. The radial artery was stripped (Fig. 2) and ligated at the distal end. Ulnar artery ultrasonography showed triphasic blood flow. The surgical wound was closed after achieving adequate hemostasis. The patient was discharged from the hospital after 3 days on medical management and follow-up advice.

- Right radial artery exploration distally found congregation of radial artery and subcutaneous tissue around catheter
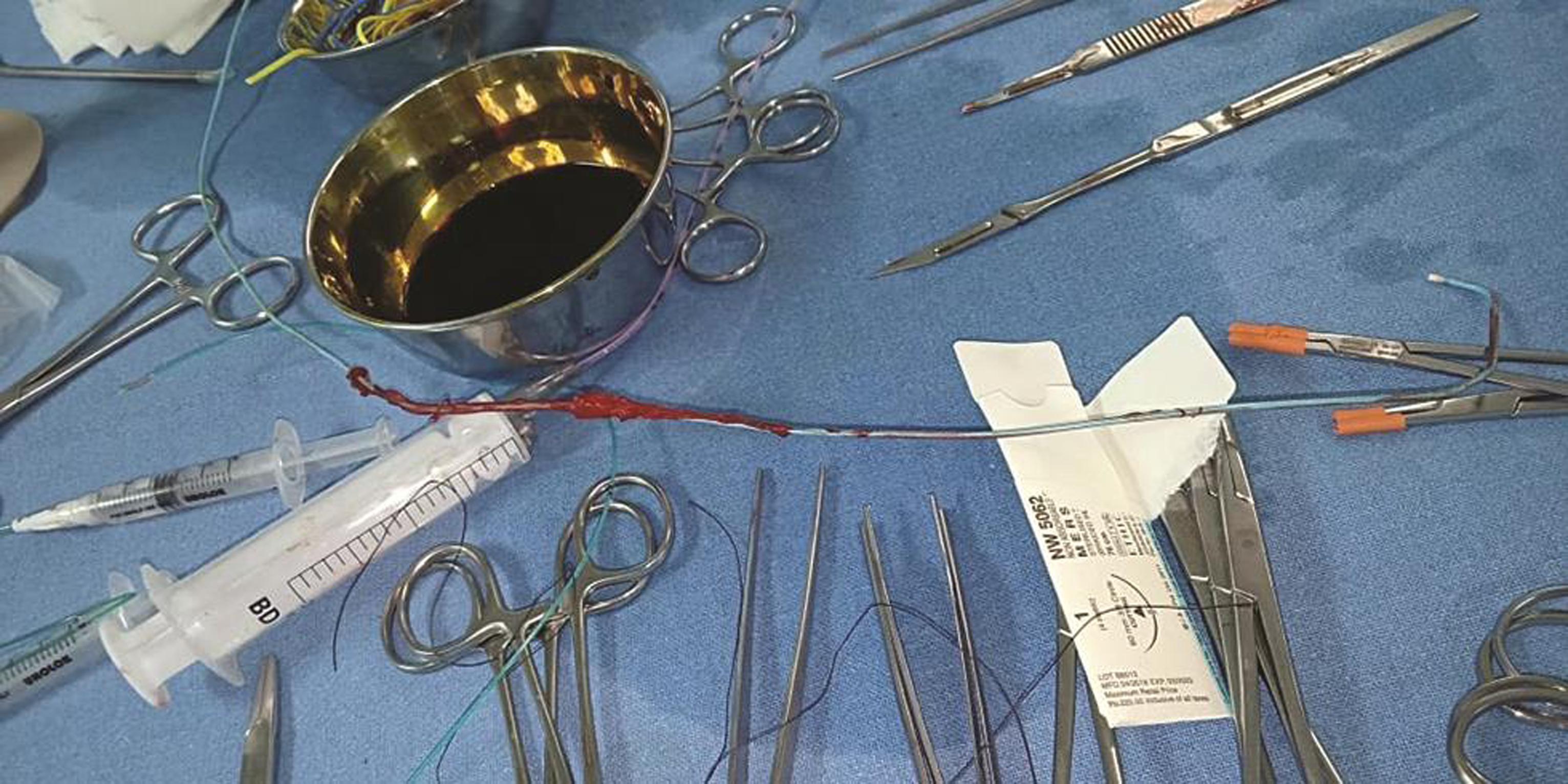
- Avulsed radial artery over the 5-Fr.
The radial artery is being increasingly used for interventional procedures worldwide because of lower incidence of access site bleeding and early mobilization of the patient, leading to decreased morbidity and lesser hospital stay. Radial artery catheterization can lead to complications such as local site bleeding, forearm hematoma, fistula formation, pseudoaneurysm, radial artery occlusion, vasospasm, and sterile abscess. Radial artery avulsion due to intense vasospasm has been described, though it is rare. Ischemic injury or damage to the hand is rare in patients with prolonged cannulation of the radial artery in critically ill patients, though the radial artery may get occluded. This is because of the dual blood supply of the hand by the radial and ulnar arteries and the palmar arch.1, 2, 3 Bedford concluded that percutaneous cannulation of the radial artery for 1 to 10 days has generally been free of serious complications, although arterial occlusion may occur in 10 to 30% cases.4
Vasospasm generally occurs in the tortuous segments and more so if there is excessive manipulation. Excessive manipulation or use of force can lead to vasospasm, which can cause radial artery avulsion, as it happened in our case.
Conflict of Interest
None declared.
References
- A randomized comparison of percutaneous transluminal coronary angioplasty by the radial, brachial and femoral approaches: the access study. J Am Coll Cardiol. 1997;29(6):1269-1275.
- [Google Scholar]
- Long-term radial artery cannulation: effects on subsequent vessel function. Crit Care Med. 1978;6(1):64-67.
- [Google Scholar]




