
Translate this page into:
Role of Thoracic Epidural Analgesia in Cardiac Surgery in Patient with Severe Scoliosis
Chinmaya Nanda, MD, FIACTA Institute of Critical Care and Anesthesia, Medanta The Medicity Sector 38, Gurgaon 122001 India nandachinu@gmail.com
This article was originally published by Thieme Medical and Scientific Publishers Private Ltd. and was migrated to Scientific Scholar after the change of Publisher.
Thoracic epidural anesthesia (TEA) has been used in high-risk cardiac surgical patients as an adjunct to general anesthesia.1 Epidural anesthesia has improved analgesia and outcomes after cardiac surgery.2 We report here a case of severe scoliosis who underwent mitral valve replacement under general anesthesia plus high TEA.
A 22-year-young female, a known case of Marfan syndrome came to us with severe mitral regurgitation due to mitral valve prolapse for mitral valve replacement. Her height and weight was 172 cm and 35 kg, respectively. Preoperative examination revealed she had a severe scoliosis with convexity toward right side (Fig. 1). Her pulmonary function test showed severe restrictive lung disease with forced expiratory volume in 1 second (FEV1) which was 1.43 L (43% predicted) and FEV1/FVC% (forced vital capacity percent) was normal.
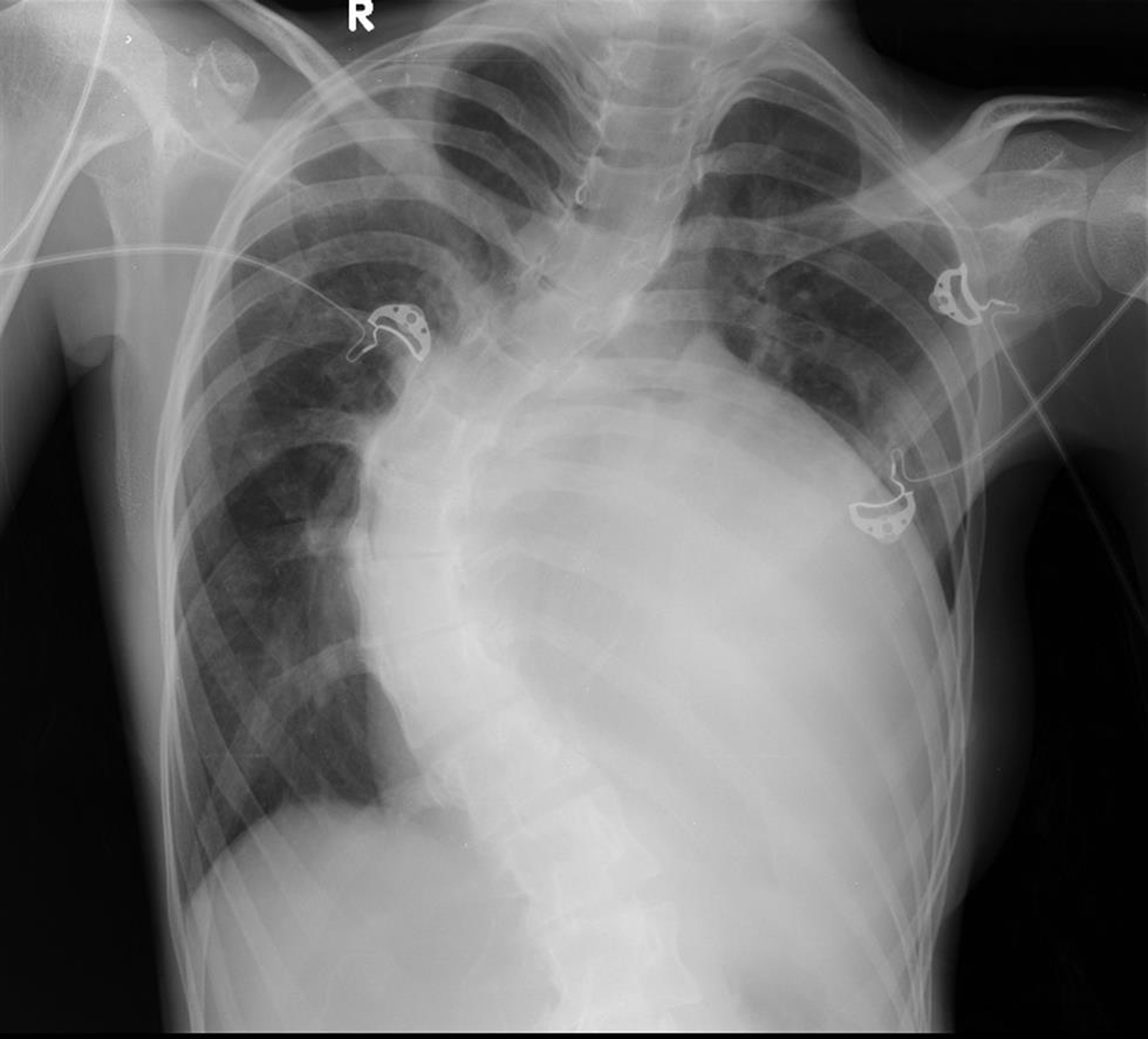
- Chest X-ray showing severe scoliosis.
In view of her poor pulmonary status, a thoracic epidural catheter was placed at the level of T1-T2 by hanging drop technique night before surgery. The next day she underwent mitral valve replacement with a bioprosthetic valve. Postoperatively she was kept on epidural ropivacaine 0.375% infusion at 6 mL/h. She was extubated 12 hours after surgery. The epidural catheter was removed on third postoperative day.
Median sternotomy for cardiac surgery causes uncoordinated chest expansion and weakness of respiratory muscles. Patients with underlying respiratory problems are at increased risk of pulmonary complications postoperatively. Hyperreactive airway, postoperative pain, immobilization after surgery, and sedative analgesics compound the problem. Mehta et al has shown that TEA might decrease pulmonary, cardiovascular and renal complications, provide better analgesia without sedation, and allows early extubation in high-risk cardiac surgical patients.1, 3 Analgesia without sedation helps in rapid mobilization of the patients and active pulmonary rehabilitation after surgery. Hemmerling et al also demonstrated earlier extubation and oxygen withdrawal time with high TEA.4
Conflict of Interest
None declared.
References
- Epidural analgesia in high risk cardiac surgical patients. HSR Proc Intensive Care Cardiovasc Anesth. 2012;4(1):11-14.
- [Google Scholar]
- Off-pump coronary artery bypass grafting: new developments but a better outcome? Curr Opin Anaesthesiol. 2002;15(1):9-18.
- [Google Scholar]
- Thoracic epidural analgesia for off-pump coronary artery bypass surgery in patients with chronic obstructive pulmonary disease. Ann Card Anaesth. 2010;13(3):224-230.
- [Google Scholar]
- Thoracic epidural anesthesia for cardiac surgery: the effects on tracheal intubation time and length of hospital stay. Can J Anaesth. 2005;52:883.
- [Google Scholar]




