
Translate this page into:
Multidetector Computed Tomographic Imaging of the Mixed Total Anomalous Pulmonary Venous Drainage
*Corresponding author: Ajmer Singh, Department of Cardiac Anaesthesia, Medanta The Medicity, Gurugram, Haryana, India. ajmersingh@yahoo.com
-
Received: ,
Accepted: ,
How to cite this article: Singh A, Joshi S. Multidetector Computed Tomographic Imaging of the Mixed Total Anomalous Pulmonary Venous Drainage. J Card Crit Care TSS. doi: 10.25259/JCCC_22_2024
Abstract
A 1-month-old infant with worsening respiratory distress and cyanosis was found to have a combination of cardiac and supracardiac, i.e., mixed total anomalous pulmonary venous drainage (TAPVD) or as it is called a type IV TAPVD. Multidetector computed tomographic imaging was done to corroborate the diagnosis and it provided precise anatomic information and correct pre-operative diagnosis for pre-surgical planning. A brief description case is described.
Keywords
Echocardiography
Multidetector computed tomography
Total anomalous pulmonary venous drainage

INTRODUCTION
Among the four types of total anomalous pulmonary venous drainage (TAPVD), the mixed or type IV variant is the rarest and accounts for only 5% of the cases.[1] Chest radiography, echocardiography, catheter angiography, multidetector computed tomography (MDCT) angiography, and magnetic resonance imaging (MRI) are useful and complementary imaging modalities for the diagnosis of this anomaly. MDCT imaging is a reliable technology for the diagnosis and pre-surgical planning for mixed TAPVD.
CASE REPORT
A 1-month-old infant with worsening respiratory distress and cyanosis was admitted for evaluation. Two-dimensional echocardiography revealed a dilated right atrium, a dilated right ventricle, a non-restrictive ostium secundum atrial septal defect with a right to left shunt, and TAPVD. The right upper pulmonary vein (RUPV) and right lower pulmonary vein (RLPV) formed a confluence with the left lower pulmonary vein (LLPV) to communicate with the right atrium through coronary sinus (CS) with flow turbulence at the confluence-CS junction. The left upper pulmonary vein was draining cranially into the left brachiocephalic vein through a vertical vein (VV). For a clearer delineation of pulmonary venous anatomy, a 256-slice MDCT imaging was performed which showed three (upper, middle, and lower) pulmonary veins on the right side. The rest of the findings were similar to echocardiography and confirmed the diagnosis of a combined cardiac and supracardiac, i.e., mixed (type IV) TAPVD [Figure 1a and b]. The diagrammatic representation of the anomaly is shown in Figure 2. The CS was found to be unroofed during the surgical correction. The RUPV, right middle pulmonary vein, RLPV, and LLPV were rechanneled to the left atrium with a Dacron patch, and the VVbrachiocephalic vein junction was transected and anastomosed to the left atrial appendage. The patient made an uneventful recovery.
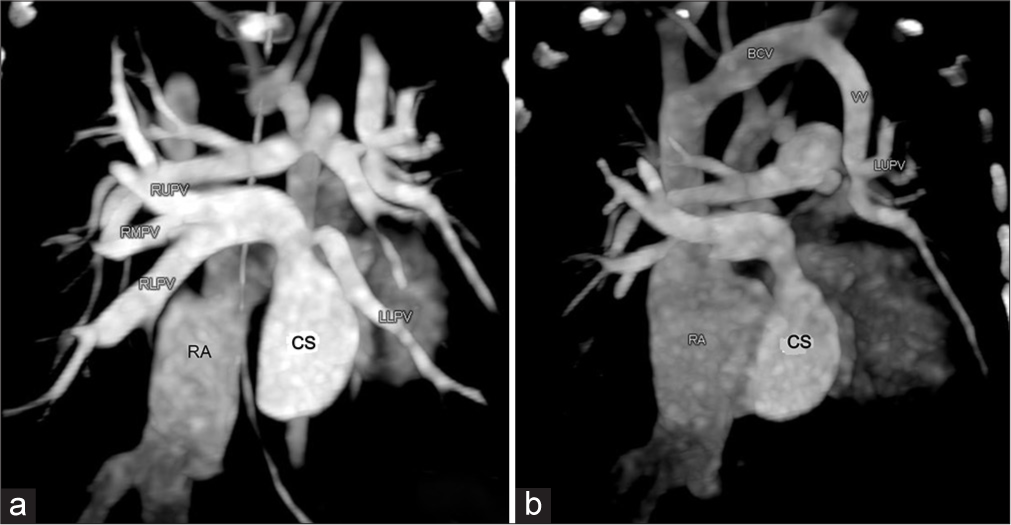
- (a) Cardiac TAPVD: MDCT axial section showing the confluence of right pulmonary veins with LLPV to drain into CS. (b) Supracardiac TAPVD: CT coronal section showing LUPV coursing cranially to drain into the left BCV through a VV. TAPVD: Total anomalous pulmonary venous drainage, MDCT: Multidetector computed tomography, RA: Right atrium, CS: Coronary sinus, RUPV: Right upper pulmonary vein, RMPV: Right middle pulmonary vein, RLPV: Right lower pulmonary vein, LLPV: Left lower pulmonary vein, LUPV: Left upper pulmonary vein, VV: Vertical vein, BCV: Brachiocephalic vein.
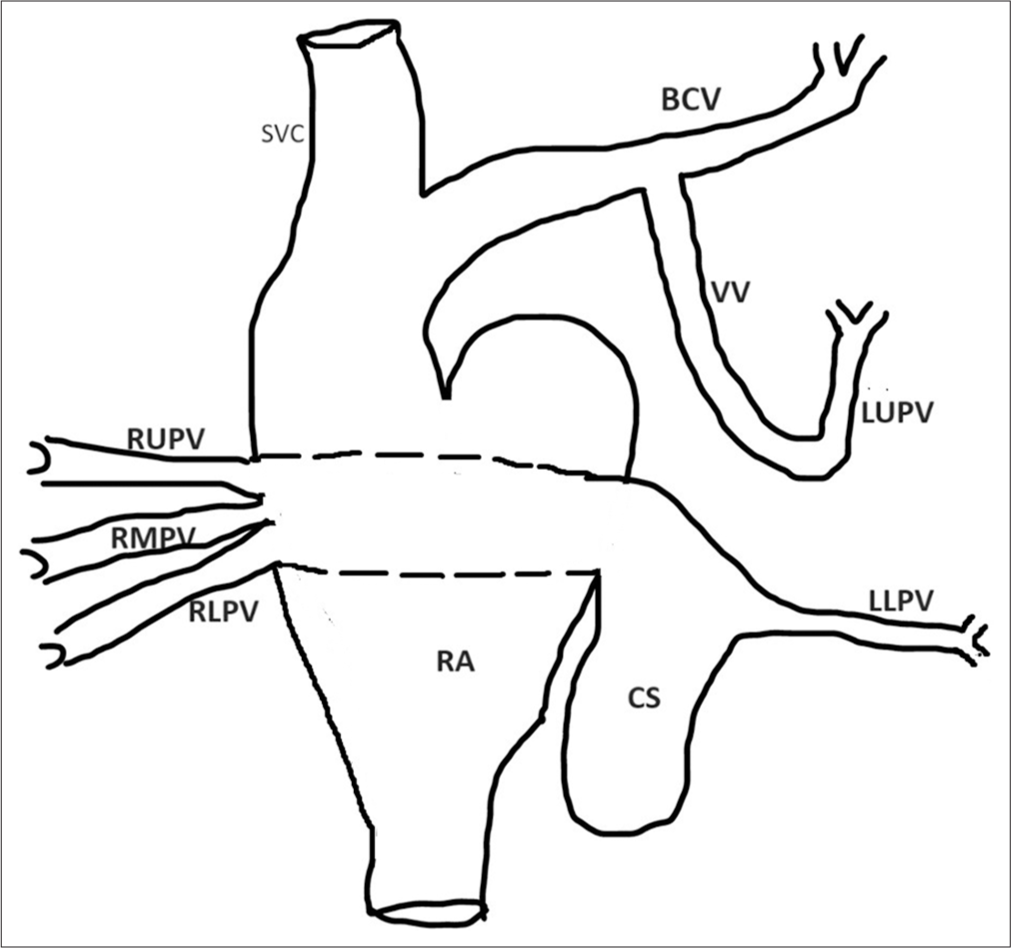
- Diagrammatic representation of mixed TAPVD. TAPVD: Total anomalous pulmonary venous drainage, SVC: Superior vena cava, RA: Right atrium, CS: Coronary sinus, RUPV: Right upper pulmonary vein, RMPV: Right middle pulmonary vein, RLPV: Right lower pulmonary vein, LLPV: Left lower pulmonary vein, LUPV: Left upper pulmonary vein, VV: Vertical vein, BCV: Brachiocephalic vein.
DISCUSSION
TAPVD is a rare, inborn cardiac abnormality in which all four or sometimes five pulmonary veins drain into the brachiocephalic vein, superior vena cava, inferior vena cava, right atrium, or CS. The reported incidence of TAPVD is 7–9/100,000 live births, and among the four types of TAPVD, the mixed or type IV variant accounts for only 5% of cases.[1] Mixed variety, additionally, is categorized into two groups: the “3 + 1” group, in which the heart or systemic veins receive three pulmonary veins and another site receives the remaining vein. In the second, “2 + 2” group, the pulmonary veins from both sides combine and connect with the systemic venous drainage at separate sites.[2] Excessive pulmonary blood flow from the anomalous pulmonary veins can cause right heart overload and pulmonary hypertension. Obstruction of the pulmonary venous return can also cause pulmonary hypertension in patients with TAPVD.[3-5]
Echocardiography is the basic and preferred imaging method for the diagnosis of pulmonary venous anomalies, but it has the limitations of a small field of view and poor acoustic window. MDCT is superior to echocardiography for the depiction of peripheral structures of the thoracic cavity, rapid image acquisition, high spatial resolution, and multiplanar reformatting capabilities. The potential advantages of MDCT over spiral computed tomography (CT) include high acquisition speed and acquisition of volume data instead of individual slice data.[6] In addition, the radiation exposure to the patient is less with MDCT compared to spiral CT. Reconstructed images from the axial and three-dimensional view are invaluable for the depiction of anomalous pulmonary venous structures. The foremost conundrums in the management of these patients center around the correct pre-operative diagnosis, accurate anatomic description, and technical issues related to surgical repair.[7] Contrast-enhanced MRI and MDCT are especially helpful in the characterization of a mixed variety of TAPVD. They provide precise anatomical information for presurgical planning and post-surgical follow-up.[8] The MRI scores over MDCT in providing more accurate tissue characterization, providing anatomic as well as hemodynamic data, and avoiding ionizing radiation.
CONCLUSION
The advantages of MDCT over MRI include faster acquisition speed, high spatial resolution, high-quality imaging, improved three-dimensional post-processing, non-invasiveness, less or no need for sedation, less expensive, and less interference by metal artifacts. MDCT imaging can provide a detailed anatomic description of the mixed TAPVD, which is essential for pre-operative planning and surgical repair.
Ethical approval
Institutional Review Board approval is not required.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation:
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
Financial support and sponsorship: Nil.
References
- Total Anomalous Pulmonary Venous Connection: Morphology and Outcome from An International Population-Based Study. Circulation. 2010;122:2718-26.
- [CrossRef] [PubMed] [Google Scholar]
- Mixed Total Pulmonary Venous Drainage: Still a Surgical Challenge. J Thorac Cardiovasc Surg. 1996;112:1581-8.
- [CrossRef] [PubMed] [Google Scholar]
- Case Report: Thoughts on Two Cases of Total Anomalous Pulmonary Venous Connection Complicated with Pulmonary Artery Hypertension. Front Cardiovasc Med. 2023;10:1075168.
- [CrossRef] [PubMed] [Google Scholar]
- Dual Drainage of TAPVR-An Exquisite Connection. J Card Crit Care TSS. 2021;5:174-5.
- [CrossRef] [Google Scholar]
- Prospective Interventional Cohort Study Using AIIMS Simplified POC Algorithm for Restricted Blood Transfusion in Cyanotic Children. J Card Crit Care TSS. 2024;8:195-204.
- [CrossRef] [Google Scholar]
- Milestones in CT: Past, Present, and Future. Radiology. 2023;309:e230803.
- [CrossRef] [PubMed] [Google Scholar]
- Mixed Total Anomalous Pulmonary Venous Connection: Anatomic Variations, Surgical Approach, Techniques, and Results. J Thorac Cardiovasc Surg. 2008;135:106-16.
- [CrossRef] [PubMed] [Google Scholar]
- Multidetector Computed Tomography (MDCT) Angiography Evaluation of Total Anomalous Pulmonary Venous Connection. Cureus. 2023;15:e46852.
- [CrossRef] [PubMed] [Google Scholar]




