
Translate this page into:
Is TEE a Game Changer in Aortic Prosthetic Paravalvular Leak?
Devishree Das, MD Department of Cardiac Anaesthesia, CT Center, All India Institute of Medical Sciences New Delhi 110029 India devishreedas111@gmail.com
This article was originally published by Thieme Medical and Scientific Publishers Private Ltd. and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Valve prosthesis have played an important role in the management of patients with valvular heart disease. However, the prosthetic heart valves used are not without complications. Almost all prosthetic heart valves are obstructive compared with native valves and associated with physiological washing jets. Because of shielding and artifacts it is very difficult to assess the prosthetic valve with TTE. Multiple thrombi and aortomitral continuity detection is cumbersome by TTE. Multiple angulations and off axis view in TEE help not only to characterize the prosthetic heart valve but also gives a three-dimensional surgical view to aid in reaching a diagnosis.
Keywords
TEE
Aortic prosthetic valve leak

Introduction
Valve prosthesis have played an important role in the management of patients with valvular heart disease. However, the prosthetic heart valves used are not without complications. Almost all prosthetic heart valves are obstructive compared with native valves and associated with physiological washing jets. Because of shielding and artifacts it is very difficult to assess the prosthetic valve with transthoracic echocardiography (TTE). Multiple thrombi and aortomitral continuity detection is cumbersome by TTE. Multiple angulations and off axis view in transesophageal echocardiography (TEE) help not only to characterize the prosthetic heart valve but also gives a three-dimensional (3D) surgical view to aid in reaching a diagnosis.
Echo Report
The TTE finding of a 69-year-old female with prosthetic aortic valve endocarditis who had undergone aortic valve replacement with #23 epic bioprosthetic valve one month before and had shown severe valvular aortic regurgitation with mild paravalvular leak, diastolic flow reversal on descending thoracic aorta, and a 18 × 15 mm mobile mass attached to the aortic valve. There was moderate tricuspid regurgitation (TR) with right ventricular systolic pressure (RVSP) being RAP+55. Inferior vena cava (IVC) was dilated and <50% collapsing and the ejection fraction (EF) was 55%.
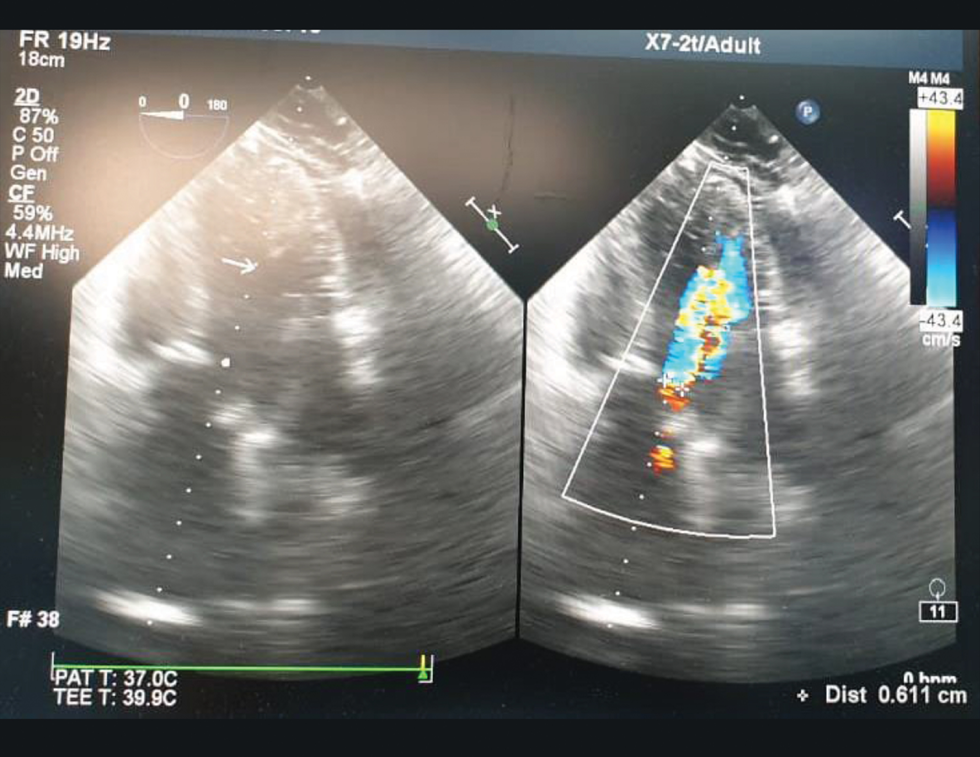
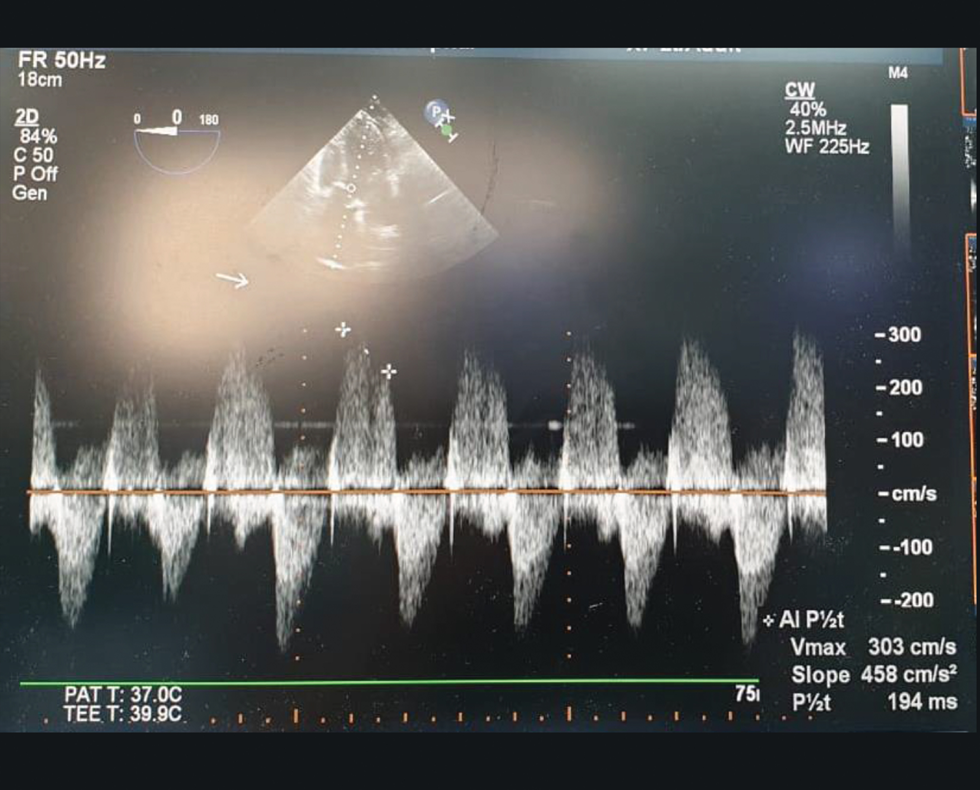
The patient was hemodynamically unstable with requirement of inotropes increased and taken to operating room for emergency aortic valve replacement (AVR). Intraoperative TEE showed prosthetic aortic valve with severe valvular AR and paravalvular leak (Fig. 1). There was a mobile vegetation (Fig. 2) attached to the aortic valve and moving toward the left ventricular outflow tract (LVOT). The aortic annulus was 23 mm while ascending aorta measured 41 mm (Fig. 3). The regurgitant jet width compared with root is >60% (Fig. 4) while the PHT was 136 msec (Fig. 5). TEE showed 0.5cm width pericardial effusion on the posterior left ventricle (LV) wall (Fig. 6). There is significant left ventricular hypertrophy (LVH) and EF was 45 to 50% (Fig. 7). Postoperatively echo showed new well-functioning prosthetic aortic valve with aortomitral continuity (Fig. 8).
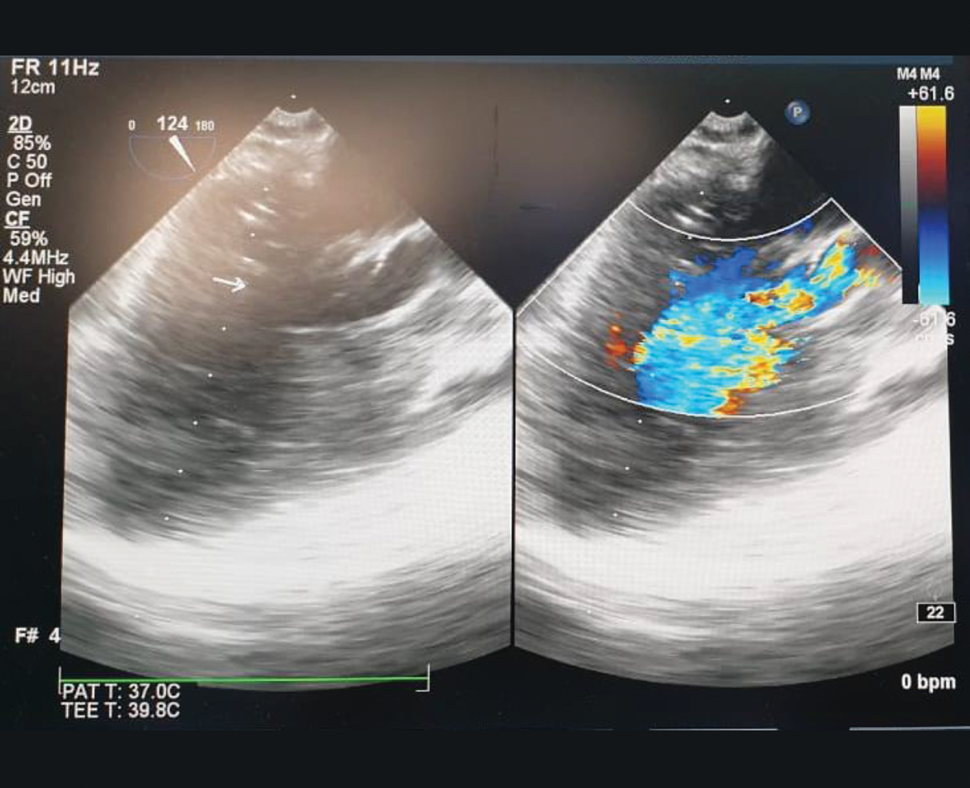
- Midesophageal aortic valve long axis view showing valvular regurgitation and paravalvular leak.
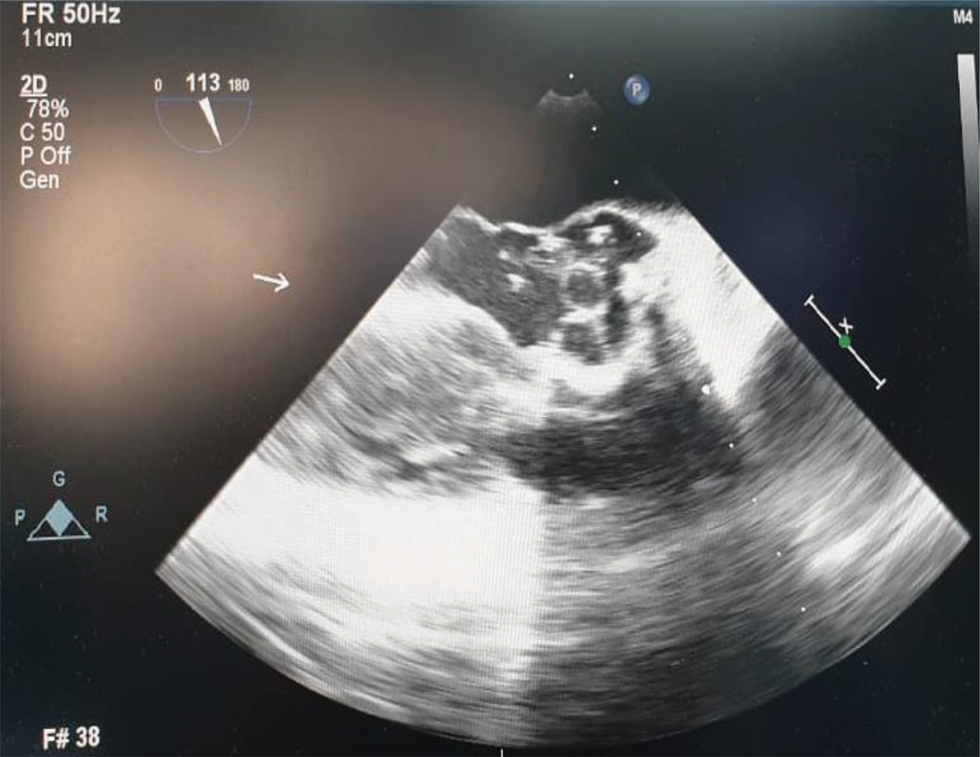
- Midesophageal aortic valve long axis view demonstrating multiple thrombi in the prosthetic aortic valve.
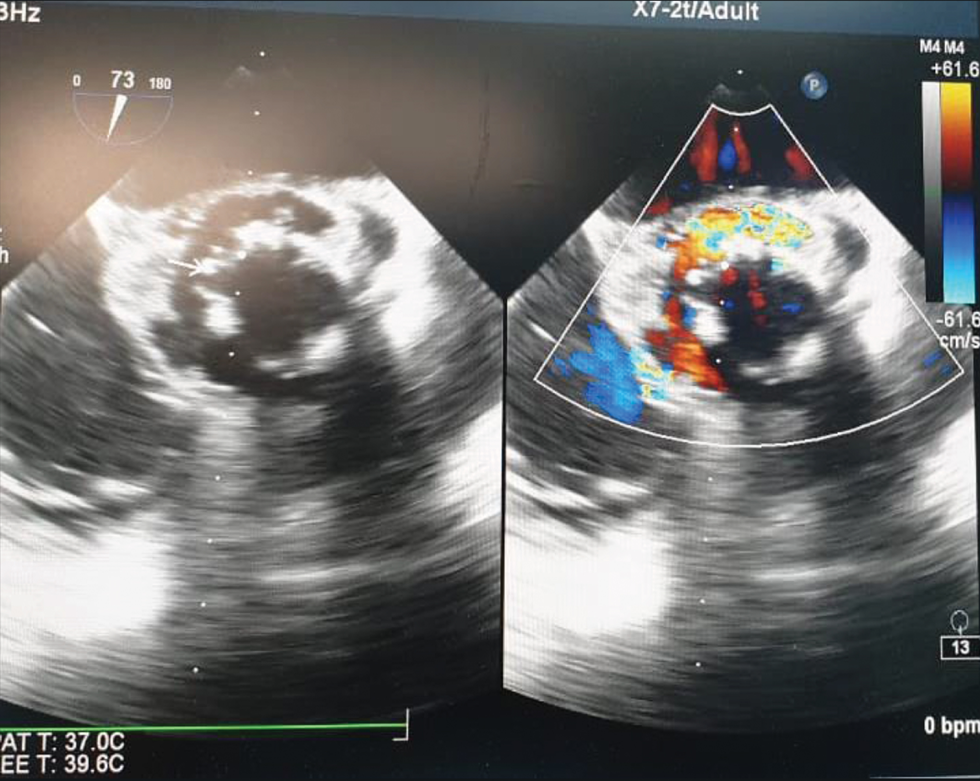
- Midesophageal aortic valve long axis view measuring the aortic annulus and proximal ascending aorta.
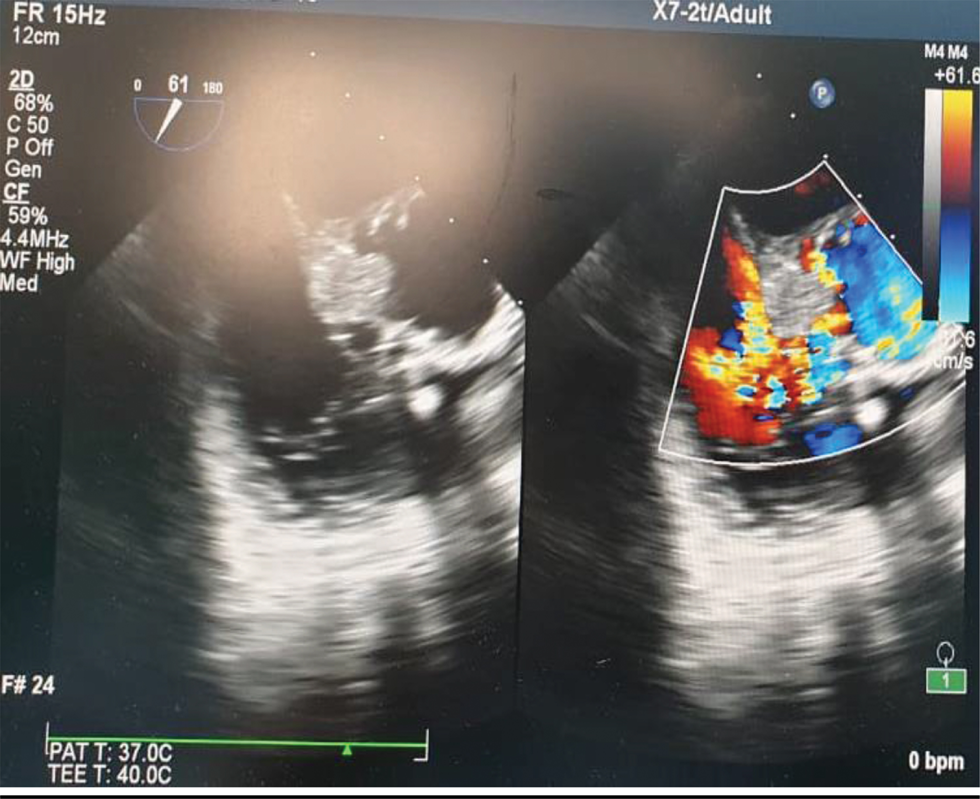
- Color M mode assessment of aortic regurgitation.
- Pressure half time for assessment of regurgitant severity.
- Pericardial effusion around LV posterior wall.

- TEE showing calculation of ejection fraction (EF).

- Midesophageal aortic valve long axis view showing prosthetic aortic valve with aortomitral curtain.
Discussion
Paravalvular leak in prosthetic aortic valve endocarditis has a grave prognosis. Mortality remains high in such cases. Intraoperative Doppler echocardiography can help in its prognostication. The parameter assed include pressure gradient, effective orifice area, and dimensionless index. Pressure gradient is assessed by simplified Bernoulli equation where pressure gradient is 4v.2 Effective orifice area has been shown to be a better index of valve function which is measured by continuity equation. Dimensionless index is the ratio of velocity proximal to the valve and the velocity through the valve. TEE gives information about multiple thrombi and helps in patient outcome. Therefore, the dynamic use of intraoperative TEE in assessing in prosthetic heart valve function especially in aortic location cannot be ignored.1-5
Conflict of Interest
None.
References
- Very long-term outcomes of the Carpentier-Edwards Perimount valve in aortic position. Ann Thorac Surg. 2015;99(3):831-837.
- [Google Scholar]
- Prevalence and clinical significance of incidental paraprosthetic valvar regurgitation: a prospective study using transoesophageal echocardiography. Heart. 2003;89(11):1316-1321.
- [Google Scholar]
- Natural history of early aortic paraprosthetic regurgitation: a five-year follow-up. Am Heart J. 1999;138:351-357. (2 Pt 1)
- [Google Scholar]
- Recommendations for evaluation of prosthetic valves with echocardiography and Doppler ultrasound. a report from the American Society of Echocardiography’s Guidelines and Standards Committee and the Task Force on Prosthetic Valves, developed in conjunction with the American College of Cardiology Cardiovascular Imaging Committee, Cardiac Imaging Committee of the American Heart Association, the European Association of Echocardiography, a registered branch of the European Society of Cardiology, the Japanese Society of Echocardiography and the Canadian Society of Echocardiography, endorsed by the American College of Cardiology Foundation, American Heart Association, European Association of Echocardiography, a registered branch of the European Society of Cardiology, the Japanese Society of Echocardiography, and Canadian Society of EchocardiographyJ Am Soc Echocardiogr. 2009;22(9):975-1014.
- [Google Scholar]
- Outcome of mild periprosthetic regurgitation detected by intraoperative transesophageal echocardiography. J Am Coll Cardiol. 2001;38(1):163-166.
- [Google Scholar]




